
- Date:
- 1 May 2022
This is the third of seven topic-based reports, as outlined in the Family Violence Reform Implementation Monitor's plan for 2021–2022.
This report examines the implementation progress in supporting workforces in universal health, and education services to identify and respond
to family violence, and government planning for the service system responses to increased identification.
Monitoring Victoria's Family Violence Reforms: Early identification of family violence within universal services
Monitoring context
About the Family Violence Reform Implementation Monitor
The Family Violence Reform Implementation Monitor (the Monitor) was formally established in 2017 as an independent statutory officer of the Parliament after the Royal Commission into Family Violence released its report in 2016. The role is responsible for monitoring and reviewing how the Victorian Government and its agencies deliver the family violence reforms as outlined in the government’s 10-year implementation plan Ending Family Violence: Victoria’s Plan for Change.
On 1 August 2019, former Victorian Corrections Commissioner Jan Shuard PSM, was appointed as the Monitor under section 7 of the Family Violence Reform Implementation Monitor Act 2016. Jan took up her role on 2 October 2019, replacing Tim Cartwright APM, the inaugural Monitor.
Monitoring approach
The Monitor’s 2021–2022 plan was developed through a process of consultation with government and sector stakeholders. Topics were selected that aligned areas of greatest interest and concern to sector stakeholders, with reform implementation activity outlined in the government’s second Family Violence Reform Rolling Action Plan 2020–2023. In determining topics, the focus was on areas where an independent perspective could add the most value to the ongoing reform effort.
Topics selected for monitoring throughout 2021 and 2022 are:
- accurate identification of the predominant aggressor
- family violence reform governance
- early identification of family violence within universal services
- primary prevention system architecture
- Aboriginal-led primary prevention and early intervention
- crisis response model for victim survivors
- service response for perpetrators and people using violence within the family.
In undertaking our monitoring, the following cross-cutting themes are examined across all topics:
- intersectionality
- children and young people
- Aboriginal self-determination
- priority communities such as LGBTIQ+, people with disabilities, rural and regional, criminalised women, older people and refugee and migrant communities
- data, evaluation, outcomes and research
- service integration.
Monitoring of the selected topics is based on information gathered through:
- consultations with government agency staff
- consultations with community organisations and victim survivor groups
- site visits to service delivery organisations
- attendance at key governance and working group meetings
- documentation from implementation agencies, including meeting papers and records of decisions by governance bodies
- submissions made to the Monitor in 2020 by individuals and organisations (many of these are available in full on the Monitor’s website.
Engaging victim survivors in our monitoring
We are also actively seeking to include user experience and the voices of victim survivors in our monitoring. The office is working with established groups including the Victim Survivors’ Advisory Council, Berry Street’s Y-Change Lived Experience Consultants, and the WEAVERs victim survivor group convened by the University of Melbourne.
Stakeholder consultation
The Family Violence Reform Implementation Monitor would like to thank the following stakeholders for their time in monitoring this topic:
- Aboriginal Community Elders Services
- Bendigo Health
- Berry Street Y-Change Lived Experience Consultants
- Centre for Excellence in Child and Family Welfare
- cohealth
- Department of Education and Training
- Department of Health
- Drummond Street
- Early Childhood Australia
- Eastern Metropolitan Regional Family Violence Partnership
- Family Safety Victoria
- Gippsland Family Violence Alliance
- Goulburn Valley Health
- Municipal Association of Victoria
- No to Violence
- Preston High School
- Royal Australian College of General Practitioners
- The Royal Women’s Hospital
- Safe and Equal
- Safe Steps Family Violence Response Centre
- Sexual Assault Services Victoria
- Seniors Rights Victoria
- Statewide Family Violence Integration Advisory Committee
- Switchboard – Rainbow Door
- Thorne Harbour Health
- Uniting Vic.Tas
- The University of Melbourne
- Victim Survivors’ Advisory Council Chair and Deputy Chair
- Victorian Aboriginal Community Controlled Health Organisation
- Victorian Council of Social Service
- Victorian Principals Association
- WEAVERs lived experience group
- Women with Disabilities Victoria.
We also thank and acknowledge the victim survivors who shared their experiences of family violence responses in health and education services. Hearing about these experiences – which are featured throughout the report, with names changed to protect individuals’ privacy – has made an invaluable contribution to our analysis.
Foreword

Jan Shuard PSM
Family Violence Reform Implementation Monitor
This report examines the implementation progress in strengthening universal health and education workforces to identify and respond to family violence early to support the safety of victim survivors. It is the third of our topic-based reports and focuses on mainstream services and their preparedness for the start of the phase 2 rollout of the Multi-Agency Risk Assessment and Management (MARAM) Framework and information sharing reforms, which occurred in April 2021.
The size and scope of this undertaking should not be underestimated, and the commitment organisations have shown is commendable. This is particularly impressive given the context of the enormous demands on these services as they responded to the impacts of the coronavirus (COVID-19) pandemic. We saw dedicated efforts in health and education sectors to improve their workforces’ ability to identify family violence and better assist victim survivors. This is despite the pressures of COVID-19, reform fatigue, uncertainty of funding and limited time available for training those delivering frontline services.
Victim survivors emphasised the importance of universal services being properly skilled in this area. They talked about the power of a GP, teacher or nurse planting the seed that helped them realise that their experience was family violence, even when they were not ready to address it at that moment. Conversely, how disempowering it was to have their situation minimised or missed.
I was particularly inspired by the hospital representatives we met with, all of whom demonstrated great passion for ensuring their services were safe and trauma-informed places for both patients and staff who have lived experience of family violence. They were very clear about every single hospital employee having a role to play in the identification of family violence. Despite only being prescribed in April 2021, hospitals are well on their way to full alignment with MARAM, likely due to the exceptional foundation that the Strengthening Hospital Response to Family Violence initiative has provided.
Once again, our work has been enriched by the expertise of our victim survivor colleagues who have led our consultations and skilfully guided the conversations with women with lived experience. Their generosity, leadership and knowledge add such depth and value to our work. As one participating victim survivor shared: ‘This is the most anyone has ever wanted to know about what is and isn’t working’. In the wise words of the Chairperson and Deputy Chairperson of the Victim Survivors’ Advisory Council:
‘We believe that listening is an act of justice and curiosity is a sign of respect. Feeling heard and respected can assist in healing and we believe this work has played a role in that.’
As with all our reports we have been greatly supported by the government agencies and the service sector that have provided the relevant materials, given their time preparing and participating in our consultations and for their thoughtful considerations and feedback on our draft reports.
MARAM is a major reform that requires whole-of-government effort – it takes time to implement and embed this in practice. This report identifies areas where, with added attention, the reform efforts would be enhanced by building on what is already being done. We hope this report is a useful reference as all parts of the system work together to plan the next stage of work.

Jan Shuard PSM
Family Violence Reform Implementation Monitor
Introduction
We know that many victim survivors may not yet have reached out to specialist family violence services but are in regular contact with universal health and education services such as early childhood services, schools, maternal and child health services, general practitioners (GPs) and hospitals. Perpetrators and people using violence are also often in regular contact with these services. As emphasised by the Royal Commission, staff in these services have a unique opportunity to identify family violence early to support the safety of victim survivors.
This report examines the implementation progress in supporting workforces in universal health and education services to identify and respond to family violence. In looking at this topic, we set out to examine:
- how well staff in these services are able to recognise the signs of family violence among clients (and staff), sensitively initiate a conversation about this and respond appropriately (including, for example, seeking secondary consultations, referring clients, and sharing information)
- the resources in place to support these workforces and the extent to which they meet workforce needs
- the effectiveness of the Multi-Agency Risk Assessment and Management Framework (MARAM) rollout in creating an integrated system for identifying and responding to family violence, and whether there has been sufficient planning for the expected increased demand on family violence services
- whether appropriate monitoring and feedback loops have been put in place to measure progress in building family violence capability within universal services and the impact on the specialist service system.
We note that staff in universal services also have a role in supporting perpetrator accountability by identifying signs that people may being using family violence. However, given the relative recency of the release of MARAM perpetrator guidance by Family Safety Victoria, the fact that training is not yet available, and tailored guidance for universal services has not yet been developed, this has not been a focus within our report.
In looking at this topic, we acknowledge that the start of the phase 2 rollout of MARAM and information sharing reforms occurred in April 2021, in the middle of the COVID-19 pandemic. Over a two-year period, the pandemic has placed enormous pressure on universal services, which have had to adapt their service models, respond to health system demands and continue to provide education and care to children and young people using adapted service models and in a way that minimised spread of the virus. In this context, the commitment demonstrated by organisations and the progress made deserve extra recognition.
Scope
For practical purposes, we have attempted to limit the scope of this analysis to mainstream settings where there are true universal (that is, freely available to all) services in the health and education sectors. We have focused our attention on GPs, schools, hospitals, early childhood education and care, and maternal and child health service providers.
Nevertheless, the findings raise issues and considerations that we expect are relevant to a broader range of services that we haven’t been able to look at for this report, such as housing, alcohol and other drugs, mental health and aged care services.
We also suggest that further consideration be given to how to engage other sectors that are not prescribed under MARAM or information sharing legislation. For example, the Y-Change Lived Experience Consultants reminded us that some young people who are experiencing family violence may, for a range of reasons, not be engaged with education; therefore, other settings such as social and community groups, and sporting clubs, could have a role to play in identifying risk factors. Similarly, we know that pharmacies were a key point of contact during the pandemic restrictions.
Language in this report
Throughout this report we use the terms ‘MARAM Framework’ and ‘MARAM’ interchangeably to refer to Victoria’s Family Violence Multi-Agency Risk Assessment and Management Framework. We use the term ‘perpetrator’ to describe people who use family violence; however, we acknowledge that Aboriginal people and communities may prefer to use the term ‘person using violence’.
Key findings and suggested actions
Consultations revealed a shared understanding of the importance of mainstream health and education services being able to identify the signs of family violence and appropriately acknowledge and respond to disclosures. Victim survivors were unanimous in wanting these services to be able to sensitively ask questions about possible family violence, explaining that even if a victim survivor is not ready to disclose, these questions can help them realise that they are experiencing family violence, and that help might be available.
Considerable work has been undertaken and funding provided to equip staff in universal health and education services to identify and respond to family violence, and MARAM is a commendable approach to ensuring multiple workforces across numerous sectors have a shared understanding of family violence, with a clear role to play in responding to it. Our consultations revealed that while Family Safety Victoria’s MARAM materials are high-quality, workforces rely on the tailored guidance developed for their sector, where it exists, and have a strong desire for simple and practical guidance. This tailored guidance for each workforce is at various points of development.
Acknowledging that embedding MARAM in organisational practice involves long-term capability building and cultural change, and that a degree of practice inconsistency may be expected but should reduce over time, multiple themes emerged from our consultations with service providers, peak and professional associations, government departments and academics.
These themes form the following section headings in this report:
- Concerted efforts have been made to build the capacity of universal health and education workforces to identify family violence.
- There are areas of planning and modelling that could be strengthened.
- There is recognition that staff identifying family violence, particularly those with lived experience, need dedicated support from their workplace.
- A number of implementation challenges were raised that will need to be considered in the ongoing implementation effort.
- Certain cohorts face additional barriers to having family violence identified by universal services.
- There is variability in access to services after family violence has been identified.
- A clear model for secondary consultations would improve coordination and consistency.
- Ongoing monitoring of reform progress and impact is essential.
There is a considerable amount of activity already underway to implement and embed MARAM in universal services, and to coordinate services and systems to better support victim survivors. We propose consideration of the following 13 actions (Figure 1) to strengthen future activity and better support family violence identification within universal services. Most of these actions relate to areas of MARAM implementation that are underway and are our suggestions of where additional focus or effort is required within this work, particularly to ensure consistency across prescribed organisations.
While these proposed actions are presented in separate categories, they are interconnected and cannot be undertaken effectively in isolation. They require Family Safety Victoria, responsible departments and sector representatives to come together to carefully plan how the system will operate. This includes longer term consideration of what training and tailored guidance workforces need, and how secondary consultations and referrals should work.
Figure 1: Thirteen proposed actions to support family violence identification within universal services
Funding
- Allocate implementation support funding for multiple years and ensure further funding is communicated well in advance of its expiry so staff are not lost.
- Victoria advocate with the Commonwealth for the creation of Medicare items relating to family violence to support General Practitioner’s identification and management of family violence as envisioned in the National Plan.
Referrals and Secondary Consultations
- Develop high-level models for referrals and secondary consultations with input from the specialist sector, universal services sectors and family violence regional integration committees.
- Provide sector-specific advice to staff in universal services on referral and secondary consultation options with input from the specialist sector, universal services sectors, Aboriginal Community Controlled Organisations and family violence regional integration committees.
- Analyse the source, frequency and length of secondary consultations, and how they are being managed and delivered by the specialist sector, including The Orange Door network.
Guidance Material
- Ensure that prescribed organisations have appropriate trauma-informed policies and support for staff with lived experience; and track the effectiveness of existing employee wellbeing measures.
- Generate more detailed sector-specific guidance around what providing ongoing support for victim survivors within their services should look like after family violence has been disclosed, and look for opportunities to co-design this advice with victim survivors.
- Update guidance around school transitions to ensure that information pertaining to family violence risk is consistently communicated, particularly the major transitions from early childhood settings to primary school, and primary to secondary school.
Embedding MARAM
- Re-examine existing and required training for all prescribed workforces and use this to inform longer term planning for workforce training.
- Further consider what is required to embed MARAM capability among prescribed workforces including through:
- additional strategies to incentivise phase 2 workforces to engage in training, build their family violence capability and see the inherent value in doing so
- access for every prescribed organisation to some form of dedicated support for their organisational alignment with MARAM.
- In progressing with training and communication approaches for education workforces, ensure these build an awareness of what the MARAM Framework is and what it means for staff , and clearly articulate how it intersects with and differs from existing initiatives and systems.
Tracking MARAM Implementation Progress
- Actively seek frontline workforce feedback about MARAM implementation to feed into governance groups and bilateral meetings.
- Support and encourage impact-focussed data collection from a range of sources, and regularly bring together quantitative data to form a coherent and meaningful view of MARAM implementation across the system.
What did the Royal Commission say and what has changed since?
Following the Royal Commission, the Victorian Government has formalised the role of universal services through major reforms such as MARAM and the Family Violence Information Sharing Scheme
The Royal Commission into Family Violence found that universal services often lack the knowledge and expertise to identify and respond when people are experiencing family violence. Victims who are seeking help will often have regular and extended contact with universal services, so these workforces are crucial in the response to family violence. Lack of knowledge within universal systems [services] was identified as one of 11 system limitations:
Key personnel in universal systems, such as health services and schools, are not adequately equipped to recognise that family violence may be occurring and often do not know what to do when it is identified.
Consistent with this, the Royal Commission made a series of recommendations that aimed to increase the capacity of universal services to be able to identify and respond to family violence.1 These recommendations included:
- whole-of-workforce training for priority sectors – including GPs and hospital workers – that takes into account and aligns with their roles and standards of practice
- secondary consultation services to be provided to universal or non–family violence services by advanced family violence practitioner positions at Support and Safety Hubs (now known as The Orange Door network), and in the interim for specialist family violence services to be provided with additional resources so they can provide more secondary consultations to universal services
- public hospitals to be resourced to implement a whole-of-hospital model for responding to family violence, drawing on evaluated approaches in Victoria and elsewhere
- routine screening for family violence in all public antenatal settings
- engagement with specialists to ensure appropriate responses to diverse cohorts.
Since then, government’s approach to implementing these recommendations has been laid out through several government plans, commitments and legislation. For example:
- The Family Violence Protection Act 2008 and Family Violence Protection (Information Sharing and Risk Management) Regulations 2018 provided the legislative basis for MARAM and the Family Violence Information Sharing Scheme.
- Ending Family Violence: Victoria’s Plan for Change includes a long-term target that ‘workers in universal services will feel confident to identify and respond to all forms of family violence’ and references the industry plan (see below), which focuses on widespread family violence capability building.
- Building From Strength: 10-Year Industry Plan for Family Violence Prevention and Response includes as an immediate action to fund ‘the development and delivery of training to meet immediate upskilling needs. This may include training across workforces (for example, in working with perpetrators) or training that targets specific workforces with a role to play in the delivery of family violence reforms, such as … maternal and child health nurses, or early childhood educators.’
- Family Violence Reform Rolling Action Plan 2020–2023 committed to the second phase of MARAM and information sharing commencing in April 2021, which expanded the scope to a further 5,800 organisations that cover 370,000 professionals, meaning that workers in settings such as ‘primary and secondary schools … public health services and hospitals … will use MARAM as part of their work’. The rolling action plan captured the introduction of accredited MARAM training in identifying and responding to family violence designed for a range of workforces that intersect with family violence. It also acknowledged that universal services have an important role in supporting perpetrator accountability – a priority in the rolling action plan – with opportunities to identify, respond and refer people using violence.
The MARAM Framework was released in 2018. Principle 2 of the framework is that ‘professionals should work collaboratively to provide coordinated and effective risk assessment and management responses, including early intervention when family violence first occurs to avoid escalation into crisis and additional harm’. It also emphasises that ‘universal services have important roles across the spectrum of family violence early intervention, risk assessment and management’. Organisations in scope for this report that have been prescribed to use MARAM and information sharing are listed in Table 1.
Table 1: Health and education organisations referenced in this report that are prescribed under MARAM and information sharing legislation
| Phase 1 |
|
| Phase 2 |
|
Note: For a full list of prescribed organisations, refer to the Victorian Government’s website.
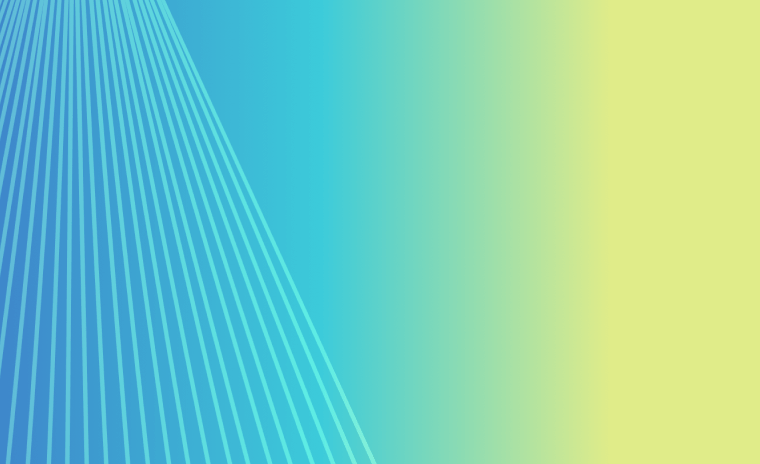
Departments are implementing MARAM together with the Family Violence Information Sharing Scheme and Child Information Sharing Scheme as a suite of interrelated reforms that work to reduce family violence and promote child wellbeing and safety. Substantial funding has been directed to these reforms, including an allocation of $97 million over four years through the 2020–21 State Budget for the continued implementation of the reforms across all prescribed workforces. The funding is designed to ‘meet the continued demand for training, change management support and information sharing from government as part of implementing the Family Violence and Child Information Sharing Schemes and MARAM, including to universal health and education workforces recently brought into these reforms under Phase 2’. A depiction of how this funding has been allocated is provided at Figure 2.
Additionally, The Orange Door network, which will be established in all 17 Department of Families, Fairness and Housing regions in Victoria by the end of 2022, is designed to be a clear point of contact for referrals and secondary consultations.
Figure 2: Flow of $97 million investment from the 2021-22 State Budget

{kind=link}
Endnotes
- We identified 11 main recommendations that directly relate to this topic: 3, 37, 95, 96, 100, 102, 103, 139, 207, 211, 212
- We understand that GPs were unable to be prescribed under MARAM because extensive sector consultation suggested they would need to be prescribed as individuals, and individuals cannot be prescribed under MARAM.
Building Capacity
Concerted efforts have been made to build the capacity of universal health and education workforces to identify family violence
The government’s self-reported progress for MARAM implementation can be found in each year's Annual Report on the Implementation of the Multi-Agency Risk Assessment and Management Framework.
Family Safety Victoria is the lead agency for the MARAM rollout and has produced an extensive suite of resources including a range of practice guidance and resources to support organisational alignment with MARAM. A summary of these documents is captured in Table 2.
As well as an extensive suite of resources, Family Safety Victoria also provides ongoing support for the agencies implementing MARAM for particular workforces through regular bilateral meetings, a MARAM implementation team available for advice, and a review and support function for all MARAM training that is developed by agencies. Family Safety Victoria has also funded Sector Capacity Building Grants to support MARAM alignment for peak bodies and leading organisations, including one-off funding to three multicultural sector organisations during the COVID-19 pandemic. Governance arrangements for the MARAM rollout include:
- the MARAM and Workforce Directors Group, which meets quarterly to oversee and provide strategic advice on the implementation of the MARAM Framework, Family Violence Information Sharing Scheme, Industry Plan and the first Rolling Action Plan of the Industry Plan
- the MARAMIS (MARAM and information sharing) and Workforce Implementation Working Group, which brings together key stakeholders from across the various sectors affected by MARAM and Family Violence Information Sharing Scheme, as well as relevant government representatives.
The 2020 Process Evaluation of the MARAM Reforms noted delays for some parts of the MARAM Framework (for example, the perpetrator guidance and guidance for working with particular cohorts) but was positive about the design of the framework and the usefulness of the practice guides:
Stakeholders reflected an appreciation of the strength of the new risk assessment approach and a recognition of the research and evidence that underpins it. In particular, the Victim Survivor practice guidance represents a comprehensive suite of practice guidance addressing all ten responsibilities defined in the MARAM Framework and provides definitive guidance based on leading evidence and practice.1
The inclusion of [the ten] responsibilities in the MARAM Framework is the first time in Victoria (or any Australian jurisdiction) that responsibilities have been specified for all organisations that intersect with family violence.2
These resources are available publicly for all prescribed organisations to use, and where tailored sector guidance doesn’t (yet) exist, government advice is for organisations to refer to the core MARAM practice guides. However, a common theme across our consultations was that the MARAM guidance was very dense and can be difficult to engage with, even sometimes for specialist services but particularly for smaller services. Implementing agencies (such as the Department of Education and Training and the Department of Health) are responsible for leading development of sector-specific training, guidance and resources that takes into account the various starting points and contextual needs of different workforces (such as the differences illustrated in Table 3 at the end of this section). We have seen substantial evidence of the range of sector-specific guidance that has been or is being developed. Workforces are overwhelmingly calling for practical and easy-to-understand guidance that explains precisely what is expected of them, provides scripts to guide conversations with potential victim survivors, and includes simple information about where to go for advice, referrals and support.
Table 2: MARAM resources available online to universal (and all) services
| MARAM Framework |
|
| Practice guide resources and tools |
|
| Organisational focused resources |
|
Source: Family Violence Reform Implementation Monitor, based on information from the MARAM practice guides and resources webpage
Hospitals
The Strengthening Hospital Responses to Family Violence (SHRFV) initiative began in 2014 as a whole-of-hospital model for responding to family violence among patients. Additional Victorian Government investment from 2016–17, provided in response to Recommendation 95 from the Royal Commission, enabled the initiative to be rolled out across the state. The model was developed by the Royal Women’s Hospital and Bendigo Health, and these two hospitals remain the sector lead hospitals for the initiative, with 27 additional hospitals funded to provide mentoring and support to the remaining services. Under the model, every hospital employee is expected to have an understanding of family violence, be trained in accordance with their position and scope of practice, and to have a role in identifying family violence.
The initiative includes training, a toolkit of customisable resources and a collaborative network for discussion and sharing of best practice. The fifth edition of the SHRFV toolkit includes alignment with MARAM and the information sharing schemes. Stakeholders spoke positively of the initiative and said it set a solid foundation for the introduction of MARAM. This is confirmed by the substantial progress in MARAM and information sharing implementation by the July to September 2021 quarter, as shown in Figure 3, despite hospitals only being prescribed in April 2021 and despite the significant pressure the hospital system has been under as a result of the COVID-19 pandemic.
Figure 3: Self-reported level of implementation of MARAM and information sharing reforms in Victorian hospitals and health services
{kind=link}
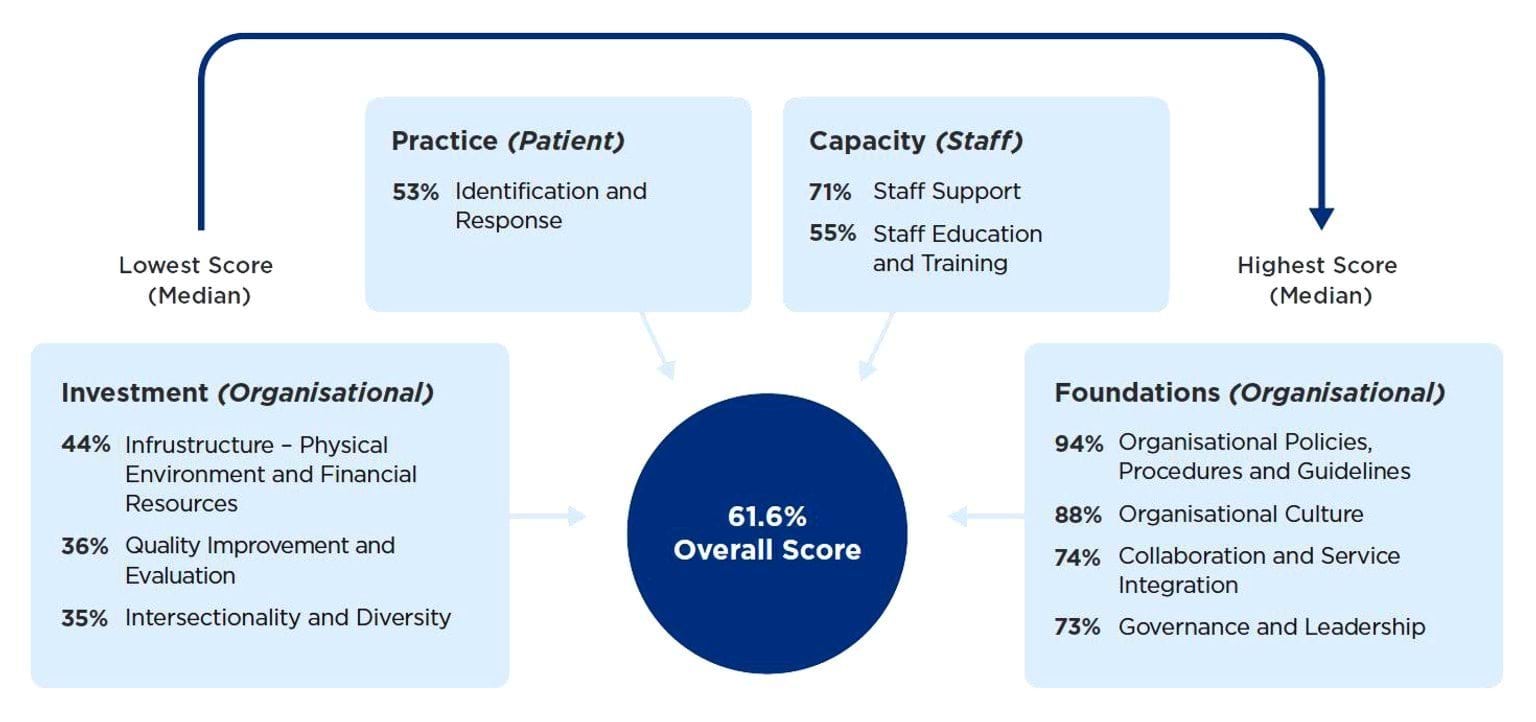
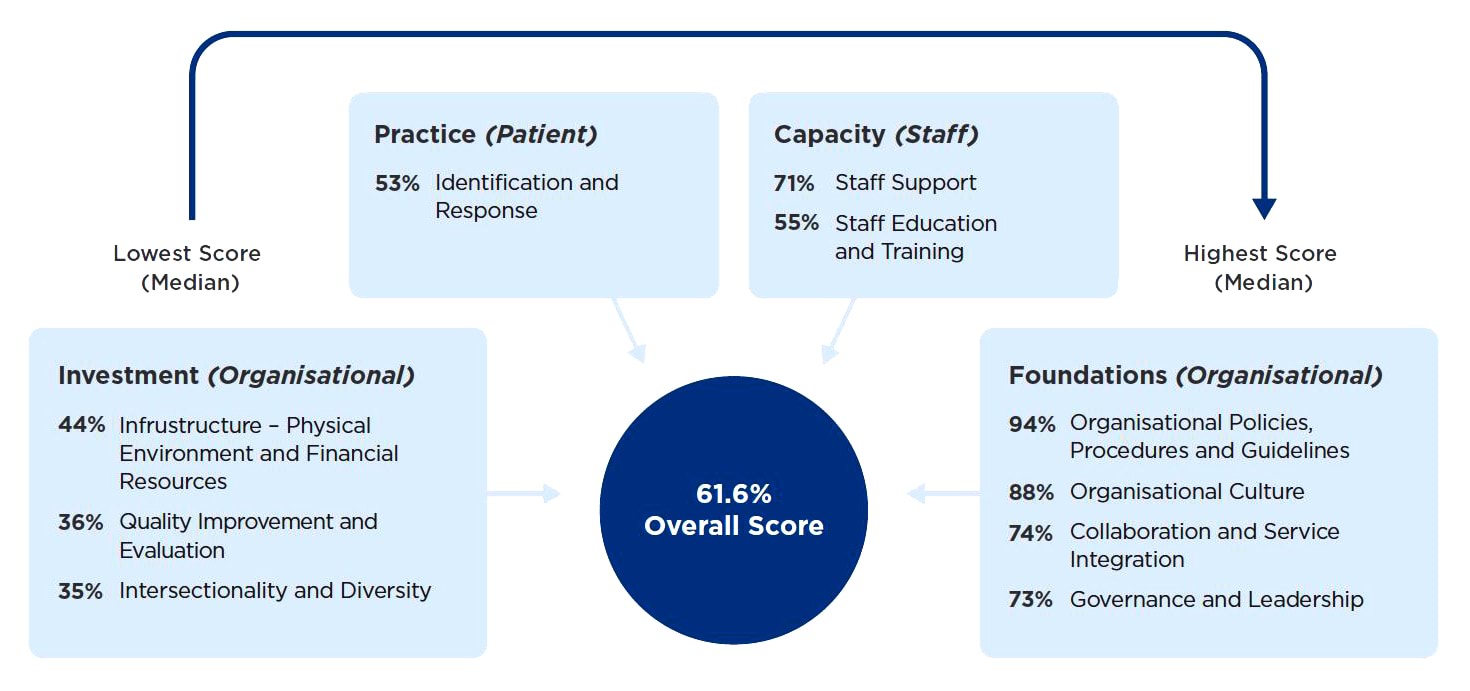
Results of the System Audit Family Violence Evaluation (SAFE) Project, which was conducted in selected hospitals and health services at three points in time across 2019 and 2021, suggest that ‘while the health services have systems in place to respond to family violence, there continues to be a need for further resourcing and improvement in a range of domains at all participating sites’.3 The audit resulted in each participating hospital achieving a score across a series of domains. High scores were achieved for foundational measures (such as having policies, procedures and guidelines in place); however, the ‘identification and response’ domain was one of the lower scoring domains (see Figure 4), indicating that more needs to be done to support hospitals to embed family violence policies in practice.
Figure 4: Statewide median score for each SAFE audit domain, from lowest to highest scores
{kind=link}
General practitioners
GPs are not prescribed under the MARAM Framework (only the information sharing schemes), but they play an important role in identifying and responding to family violence. Approximately 83 per cent of Australians see a GP at least once a year, and victim survivors are more likely to disclose to GPs over any other group, except family and friends.
The government had previously been criticised for a lack of ‘sufficient engagement with this sector’. However, in the past two years, considerable progress has been made. The University of Melbourne’s Safer Families Centre – which is leading a national, Australian Government–funded family violence training program for primary health care providers, The Readiness Program – has received funding from the Victorian Government to create a Victoria-specific, MARAM and information sharing–aligned version of the program. The Safer Families Centre convenes a MARAM and Information Sharing Advisory Group to guide this work, with representation from Family Safety Victoria, the Department of Health and the Royal Australian College of General Practitioners. Key components of the work include:
- a Victorian supplement covering MARAM and the information sharing schemes to the latest edition of the Royal Australian College of General Practitioners’ ‘White Book’ (officially titled Abuse and Violence: Working with our Patients in General Practice, 5th edition)
- development of a Victoria-focused information sharing e-learning module
- management and delivery of a virtual practice-centred intensive learning program at 22 sites.
Maternal and child health
Prescribed in phase 1 of the MARAM rollout, the maternal and child health workforce (of approximately 1,500 staff) has previously engaged in family violence training, but more recently, 1,406 maternal and child health nurses completed tailored MARAM Screening and Identification training delivered by the Centre for Excellence in Child and Family Welfare. The training focused on supporting nurses to confidently identify and respond to family violence risk and collaborate with specialist services. In addition to this, we understand a MARAM Screening and Identification eLearn package has been developed by the Department of Health for health workforces, including maternal and child health staff.
The Department of Health funds an additional maternal and child health 60-minute consultation for cases where families are experiencing or are at risk of experiencing family violence. Maternal and child health nurses are supported by a practice note that guides nurses through the consultation, including specific family violence risk assessment questions. The Department of Health was not able to provide data on the use and outcomes of these consultations.
Further resources are available through the Municipal Association of Victoria, which was funded to develop a suite of tailored practice guidance and resources for the maternal and child health workforce.
Data on the effectiveness of the maternal and child health workforce in identifying and responding to family violence is not currently available but is expected through an evaluation due to be finalised in late 2022.
Schools
The Department of Education and Training led a two-year trial across 2018 and 2019: Supporting Student Cohorts Affected by Family Violence Initiative (Family Violence Initiative). The initiative’s evaluation suggests it was highly effective, and in 2021 it received the Evidence Based Policy Award at the IPAA Leadership in the Public Sector 2020 Awards for achieving ‘significant increases in school staff members’ levels of awareness, knowledge, skill and confidence to support students affected by family violence as well as increased identification and improved referral pathways’.4 Participating schools received training and materials, clear roles and responsibilities were defined for everyone within the school and broader community, and schools and partner organisations participated in Local Area Working Group meetings.5
According to the Department of Education and Training, this initiative aimed to create a best practice process for schools to respond to family violence, noting that the whole-of-government victim survivor MARAM practice guidance had not been released and education was not yet prescribed. Anecdotally, participating schools experienced a spike in family violence identification numbers, suggesting there may be significant unmet need in schools.
Specialist roles at the regional level, and one or two staff per school, are expected to have targeted MARAM training developed for them over time to enable them to support schools as part of a differentiated workforce approach. However, the main way MARAM is currently being implemented for school-based staff is through the following measures:
- The delivery of information sharing and family violence reforms interactive webinars and eLearns. These primarily focus on information sharing obligations, and provide a brief introduction to MARAM. Schools are advised that one leader and two staff members per school should complete sessions in person or online, although more staff can be trained if desired.
- The Information Sharing and Family Violence Reforms Toolkit and Contextualised Guidance, which were developed in close consultation with education and care professionals, was designed to help organisations prepare their workplaces for implementation and provide guidance on information sharing.
- The revision of Respectful Relationships ‘responding to disclosures’ training package to align with MARAM and information sharing reforms, being undertaken in partnership with Safe and Equal. The Respectful Relationships whole-school approach (which has been adopted by almost 2,000 Victorian government, Catholic and independent schools) includes access to on-the-ground support from Respectful Relationships area staff, who are expected to have a major role in implementing MARAM in schools. This training might more suitably be named ‘identifying and responding to family violence’ training because this would better reflect the content of the training and would emphasise the active role of staff in identifying family violence.
- Content provided as part of PROTECT guidance. The guidance includes advice for schools and others about their obligations under the Child Safe Standards, Mandatory Reporting and Duty of Care and how to identify and respond to all forms of child abuse, including family violence. Staff are also required to complete Mandatory Reporting training, which covers responses to disclosures and suspicions of child abuse.
The Department of Education and Training has advised that it is drawing on key learnings from the Family Violence Initiative to inform its approach to MARAM alignment; however, there are some clear divergences from the trial in the department’s approach to MARAM implementation in schools, such as the train-the-trainer approach for Respectful Relationships disclosures training. Under this approach, Safe and Equal trains Respectful Relationships area staff, who then deliver the training to schools signed on to Respectful Relationships. However, we understand that schools’ willingness to welcome this training into the school varies and, while all school staff are invited to participate, it is not clear what proportion of staff normally attend. We also understand that the training will only be repeated or ‘topped up’ if a school requests this of area staff, yet the president of the Victorian Principals’ Association emphasised the importance of ongoing training in this area. It is also less explicit that this is a whole-of-school approach to identifying and responding to family violence, even though this is a key feature of the Respectful Relationships model and of the SHRFV model for hospitals.
Consultations with school sector representatives suggest there is still considerable progress to be made to ensure all schools know what the MARAM Framework is and to gain a clear understanding of their obligations [relates to action 11]. It will be vital to measure the impact of the approach to MARAM implementation over time, not just from the perspective of principals but also classroom teachers, wellbeing staff, administrative and other support staff, who all have a role in identifying and responding to family violence [relates to action 13]. The planned and funded evaluation of MARAM implementation in education settings will be an excellent first step in measuring effectiveness.
Early childhood education and care
The early childhood education and care sector has access to much of the same training and resources as schools. For example:
- This sector also has access to similar PROTECT guidance. Some early childhood educators working in Victorian government-funded kindergarten programs with a bachelor, diploma or certificate III qualification can access Respectful Relationships education that has been tailored for this workforce by Monash University.
- Information sharing and family violence reforms eLearning, and the Information Sharing and Family Violence Reforms Toolkit and Contextualised Guidance, are also available to this sector.
While it would have been prudent to have tailored training and resources available when organisations were prescribed in April 2021, this work is now underway through the Building Family Violence Prevention and Response Workforce Capability Project, which brings together the Department of Education and Training, Early Childhood Australia and Family Safety Victoria. Consultation with the sector has occurred, and tailored resources are being developed and will be shared with the three pilot organisations from May 2022 [relates to action 11]. The consultation report made a series of recommendations, including the need for regular communication about family violence reforms, sector-specific resources, more MARAM-related content in the available webinars and eLearns, and better promotion of the MARAM and information sharing enquiry line. Early Childhood Australia advised that through this project it will develop resources such as:
- a more streamlined family violence screening tool
- a secondary consultations flowchart for its staffroom
- a fact sheet for centre directors to use at induction with new staff.
Concurrently, the Department of Education and Training has worked with Monash University to develop and deliver training for early childhood educators on identifying family violence and responses to family violence disclosures.
Table 3: Selected ‘broader workforce’ results from the 2019–20 Census of Workforces that Intersect with Family Violence
| Community health | Early childhood | Maternal & child health |
Public health services |
Schools | |
|---|---|---|---|---|---|
| # of respondents | 328 | 136 | 135 | 565 | 82 |
| Proportion who: | |||||
| are in contact with individuals who are experiencing or at risk of family violence, at least weekly |
37% | 28% | 42% | 24% | 47% |
| are in contact with individuals who are perpetrating or at risk of perpetrating family violence, at least weekly |
23% | 9% | 12% | 15% | 20% |
| are very or extremely confident identifying family violence among... |
|
|
|
21% adults 22% CYP 15% perpetrators |
|
| are confident that they have had enough training and experience in relation to family violence response to perform their role effectively |
34% | 11% | 33% | 18% | 25% |
| want more training in (top 3 areas) |
|
|
|
|
|
Source: Family Safety Victoria.
Note: FV = family violence; CRAF = Common Risk Assessment Framework (the precursor to MARAM)
Endnotes
- Cube Group (2020): Family Safety Victoria: Process Evaluation of the MARAM Reforms Final Report (unpublished).
- Ibid.
- The Royal Women’s Hospital and the University of Melbourne (2021): The System Audit Family Violence Evaluation (SAFE) Project, Final Report, p. 4.
- State of Victoria (2021): Annual Report on the Implementation of the Multi-Agency Risk Assessment and Management Framework 2020–21, p. 14.
- Acil Allen Consulting (2020): Report to Department of Education and Training: Supporting students cohorts affected by family violence initiative, Final Report (unpublished).
Planning and Modelling
There are areas of planning and modelling that could be strengthened
With a whole-of-government reform of the scale of MARAM – which is central to many of the Royal Commission’s recommendations – planning and coordination are vital for successful implementation and service delivery.
Planning, sequencing and communication
We note that while we have seen a range of planning activity relating to phase 2 implementation, feedback from many services and sector representatives is that there is a need for very clear, practical guidance that shows what MARAM means for them. Despite the substantial lead time for the phase 2 commencement, this tailored support was not put in place before universal services were prescribed. Family violence regional integration committees, the Centre for Excellence in Child and Family Welfare and Early Childhood Australia advised that services were underprepared for being prescribed and were confused about what MARAM is. Indeed, the school principals we spoke with commented that they did not know what MARAM was until looking it up.
Around the time that schools were prescribed, and in the lead up to prescription, a range of communication methods, such as all-staff emails and social media, were used to notify schools and encourage training uptake. Individual letters from the Secretary of the Department of Education and Training were sent to schools in October 2021, providing them with a hard copy of the Information Sharing and Family Violence Reforms Toolkit; this was the first direct source of communication about schools being prescribed. In the context of the COVID-19 pandemic, communication does not seem to have penetrated.
The early childhood sector is also calling for more support. The first recommendation from the Family Violence Prevention and Response Workforce Capability Project interim report emphasised the need for stronger communication from the Department of Education and Training, with a stronger focus on MARAM.1
The intent of MARAM is for all workforces to have a shared understanding of and approach to family violence, with clear roles and responsibilities. To be able to fully participate in the system, universal services need to understand what the MARAM Framework is, and their role in the system [relates to action 11]. Now that schools and early childhood education are largely returning to normal after two years of significant disruption, we suggest an immediate focus on renewing efforts to build awareness of what the MARAM Framework means for schools and early childhood services, and clearly articulating how it intersects with and differs from existing initiatives and systems, in addition to the continued work on rolling out training.
One Principal Strategic Advisor noted that in March 2021 Family Safety Victoria provided a snapshot to all Principal Strategic Advisors of how the MARAM rollout was occurring across departments and what it was going to look like for various organisations. This was said to be a highly effective tool for communicating the big picture of the MARAM rollout. It might be worth updating this snapshot at different stages of implementation and making it available for ongoing communication with a wider audience as a way of highlighting MARAM as a whole-of-community response.
Modelling and forecasting
The only modelling or forecasting we have seen in relation to the phase 2 rollout of MARAM is in the regulatory impact statement (RIS) prepared by Family Safety Victoria. The RIS was based on consultation with a range of stakeholders including schools, early childhood centres, hospitals and health services and the Royal Australian College of General Practitioners. Consultation with a small group of phase 1 organisations also occurred to explore the potential impact on them of the phase 2 rollout. The RIS acknowledged and attempted to quantify the impact on phase 2 organisations of being prescribed under MARAM and information sharing legislation, including:
- upfront costs of staff time to participate in training
- upfront costs of updating existing policies, procedures, practice guidance, tools and systems to meet the requirements of the Family Violence Information Sharing Scheme and to align to MARAM
- ongoing costs to prescribed organisations and services associated with family violence information sharing and risk assessment and management activity (including training new staff and time spent on information sharing and family violence risk assessment and management).
We have not seen any modelling of the potential impact on specialist family violence services, both in terms of secondary consultations and referrals (which are discussed in later sections). There was consensus among non-government stakeholders that while a longer term aim of MARAM was to enable earlier intervention in family violence cases, thereby reducing pressure on the specialist family violence service system, in the short term, increased demand was to be expected. Family Safety Victoria indicated that it expected only a very gradual increase in demand over time, but we have not seen figures that confirm this is what has occurred.
Training – forecasting and strategy
Given the number of workers in services affected by the reforms, we would expect that detailed modelling around training would be required. Again, the only source of such modelling we found was in the RIS, which made assumptions about the training impact on some universal services. For example, it was assumed that across an initial three-year period:
- For hospitals – four people per organisation or service would attend one day of face-to-face training, and 25 per cent of the remainder of staff in the organisation or service would complete three hours of online training.
- For schools, early childhood education and care providers, out of school hours care, and health and support services – four people per organisation or service would attend one day of face-to-face training, and 50 per cent of the remainder of staff in the organisation or service would complete three hours of online training.
“I feel like frontline workers should do training on how to raise issues or concerns, but this training should be ongoing, it should be refreshed yearly and expanded on in terms of content and ever-changing information.”
- Kelly, victim survivor
We understand that there have been refinements to the training approach since the RIS was prepared; however, we have not seen any work to model the phased training requirements by departments. At the statewide level, there is a target of 22,000 workers being trained per year as part of the latest State Budget, and Family Safety Victoria is confident that it will exceed this target. For education workforces, Department of Education and Training guidance included a minimum readiness requirement of one leader and two professionals per organisation.
Recommendation 3 from the Royal Commission was to develop a sustained workforce and development training strategy to support MARAM. This recommendation was acquitted by the series of training-related actions included in the Strengthening the Foundations First Rolling Action Plan 2019–2022. However, a standalone training strategy is only now being developed, the content of which was accepted at the November 2021 MARAM and Workforce Directors’ Group meeting. The implementation timeline of the training strategy stretches out beyond 2029, which is consistent with Family Safety Victoria’s advice that it will be many years before all workers who require training will be trained. The strategy outlines the two sectors to deliver training:
- The specialist family violence sector delivers unaccredited training – this has been the focus of training delivered to date, acknowledging the large number of workers needing to be trained. The strategy anticipates that, ultimately, the specialist sector will best be able to leverage its unique strengths by focusing on professional development that builds on core skills and covers up-to-date MARAM content for prescribed workforces.
- The Vocational Education and Training (VET) sector delivers accredited training through Technical and Further Education institutions (TAFEs) and registered training organisations – the first of three accredited courses aligned to MARAM responsibilities is currently available. Family Safety Victoria’s long-term plan is to for a range of professions to complete their family violence accredited training as part of their pre-service qualifications. Challenges include ensuring there are enough qualified trainers to deliver the content (as flagged in the 2020 MARAM Process Evaluation of the MARAM Reforms and raised by Chisholm TAFE in our consultation with them) and advocating for family violence content to be covered in the higher education system as part of degrees for relevant workforces (this is outside the scope of the training strategy). The quality of VET trainers will increasingly be supported by the Best Practice Education Model, which provides guidance to training organisations on the essential vocational competencies for trainers so they deliver family violence courses in ways that are safe, effective, inclusive and culturally appropriate.
The currently available accredited course, Identifying and Responding to Family Violence, is designed for universal services, although it is nominally a 50-hour course spread over multiple months. The training strategy itself identifies that few current workers will self-select into this course due to barriers such as the time requirement and balancing this with other work demands. Preliminary findings from the evaluation of the accredited course suggest that while trainers report positive feedback from students participating in the unit, there are low completion rates, and many stakeholders believe the course is too long and not appropriately tailored to students’ needs. Chisholm Institute of TAFE suggested that the expertise of the TAFE sector should be used to refine the course and to develop any similar qualifications to ensure course design and content are appropriate for target audiences.
While the higher education system is not included in the training strategy, as the Victorian Government does not hold responsibility for funding and regulation, there are interdependencies given a substantial proportion of the universal services workforces have higher education (rather than VET) qualifications. For example, the training that teachers receive in universities will affect what unaccredited family violence training needs to be available for them once they have joined the workforce [relates to action 9]. It will be important for Family Safety Victoria to continue to engage with the Victorian higher education sector on the family violence reforms. There is also likely to be benefit in mapping the available pre- and post-service training available for each prescribed workforce to identify gaps and design training to meet future needs. This could include consideration of ways to incentivise MARAM-related training, such as linking it to teacher registration through the Victorian Institute of Teaching [relates to action 10].
Endnotes
- Early Childhood Australia Victoria Branch (2021): Interim Report: Building Family Violence Prevention and Response Workforce Capability Project
Support in the workplace
There is recognition that staff identifying family violence, particularly those with lived experience, need dedicated support from their workplace
MARAM resources acknowledge that ‘vicarious trauma … is a common response to working with people experiencing trauma’, that staff with lived experience of family violence are more susceptible to this vicarious trauma, and that organisations need to be prepared to support their staff in a trauma-informed way. We note that in many of our consultations, stakeholders showed they were aware that a proportion of staff in their services would have lived experience of family violence.
“Universal frontline workers also need support to deal with these issues … to decompress if they come across something personally challenging … they need support to give support.”
- Sharon, victim survivor
Research conducted by the University of Melbourne has shown that among female health professionals, there are high rates of lived experience of intimate partner violence and family violence (see Figure 5), and these rates appear to be higher than for women in the general community. For example, in 2016, 2.3 per cent of Australian women aged 18 or older had experienced intimate partner violence in the preceding 12 months, versus 11.5 per cent of women in the hospital study.
Figure 5: Experiences of intimate partner violence (IPV) and family violence (FV) among health professionals in a major tertiary hospital, 2013

Source: The University of Melbourne, based on data from McLindon E, Humphreys C, Hegarty K (2018): ‘It happens to clinicians too’:an Australian prevalence study of intimate partner and family violence against health professionals, BMC Women’s Health, 18:1123.
Stakeholders told us that, in their experience, where staff have lived experience of family violence, they have a deeper understanding of family violence and are more likely to be driven to identify and support those currently experiencing family violence, but that sometimes past trauma acts as a barrier to engagement with family violence cases because of the risk of retraumatisation.
“I feel like my lived experience really helps working with clients, for example if a client is nervous or fearful I will explore and ask questions without fear of hearing what they have to say. I can listen to a client’s story and not cry or be overly empathetic in a patronising way. I can often pick up certain behaviours that indicate family violence. My experience I feel gives me the confidence to ask the tough questions and to listen to stories (so long as I have self-care routines in place).”
- Kelly, victim survivor
The University of Melbourne research found that, overall, lived experience among health professionals seemed to contribute to better clinical care for patients experiencing family violence.
Given the potential for vicarious trauma for those exposed to secondary family violence, and the known over-representation of victim survivors within the health workforce, organisations must provide adequate support for staff. Further, MARAM alignment, and any other efforts to improve the response to victim survivors, must cover both patients/students and staff with lived experience [relates to action 6].
The 2019 Census of Workforces that Intersect with Family Violence showed that staff in universal services had access to support if they encountered family violence cases or disclosures of family violence, but views on the effectiveness of these supports were mixed, and substantially lower for school workforces (see Table 4). Further, there is no breakdown of responses by those who are victim survivors and those who are not. It would be useful to further explore the quality of support available to staff and identify ways to improve its effectiveness.
Table 4: Staff access to support regarding exposure to family violence cases from the 2019–20 Census of Workforces that Intersect with Family Violence
|
Community |
Early |
Maternal and |
Public health |
Schools | |
|---|---|---|---|---|---|
| # of respondents | 328 | 136 | 135 | 565 | 82 |
| Proportion of respondents who have access to support if they encounter cases of FV or disclosures |
93% | 89% | 97% | 91% | 83% |
| Percentage of respondents who found the support very, or extremely, effective |
61% | 66% | 61% | 58% | 38% |
Source: Family Safety Victoria
MARAM Framework guidance suggests that alignment with MARAM should include a family violence leave policy, appropriate policies and procedures and a trauma-informed approach to supporting staff who are experiencing vicarious trauma through their contact with family violence cases, particularly those staff with lived experience. There is also a workplace safety plan template available for use with an individual employee experiencing family violence, to ensure adequate workplace supports are in place.
There are also more specific supports for individual workforces. For example, the Department of Education and Training and the Department of Health promote Employee Assistance Programs for individual counselling as needed and have family violence leave available. The Strengthening Hospital Responses to Family Violence initiative includes a Family Violence Workplace Support Program, which includes training around staff disclosures and a suite of resources to help hospitals and health services better support staff who are experiencing family violence.
However, there are gaps in the coverage of this support. For example, Early Childhood Australia noted that many staff in early childhood education and care settings did not have direct clinician supervision, lacked opportunities to debrief and did not have access to an Employee Assistance Program. Similarly, one victim survivor we spoke to explained that although she worked in a public hospital, she was a casual ‘bank’ midwife (that is, she worked across multiple sites, as needed) and therefore did not have access to family violence leave.
Even where support does exist, it appears that there is a real reluctance among staff to disclose their experiences of family violence. Within the hospital study, many staff with lived experience were uneasy about accessing family violence support such as family violence leave within their organisation; their ‘primary concern was that to access leave would require disclosure to somebody in authority who might not respond with sensitivity and discretion’.
Feedback from victim survivors, including those working in universal services and even specialist family violence services, was that there is still a substantial amount of stigma associated with experiencing family violence; that victim survivors are judged as having an inherent weakness and are less desirable as an employee.
“There is still a lot of judgment, victim blaming, and shame placed upon victims of violence.”
- Lily, victim survivor
The midwife we spoke to expressed a very strong reluctance to disclose her family violence to her employee and to access the Employee Assistance Program. She did not feel that her workplace would be supportive, and she commented that in her 13 years with the employer, she would have thought she was the only one who had experienced family violence. Beth’s experience (see Beth’s experience below) is also one of feeling alone and unsupported in the workplace.
“Barely anyone [at work] knows about the family violence I am experiencing. I am very cautious of who I reveal the family violence to as I fear this will
be used against me.”
- Lily, victim survivor
“If you’re open about your situation you do get discriminated against when opportunities for progression arise.”
- Ilona, victim survivor
There is clearly a need to ensure workplaces are truly trauma informed, don’t intentionally or inadvertently discriminate against people with lived experience, and make employees feel safe to disclose if they wish to do so. The work to improve the way universal services identify and respond to family violence must extend to employees as standard practice.
Beth's experience
Beth lived in a small town with her husband, Peter. There were early signs that Beth was experiencing family violence. He contacted her constantly throughout the day, but she put it down to him demonstrating affection for his new wife.
Peter’s drinking and abuse impacted on her mental health, especially once they had children, and he made her an appointment with the local GP. He came along to the appointment where a referral to a psychologist was made, and attended the first appointment with the psychologist. Peter told Beth that he spoke to the doctor who promised to keep him updated on her progress. Because of this, she did not feel safe to speak freely to either the doctor or psychologist.
Their kids attended the local kinder and school. Beth believes there were signs that should have been questioned – like her daughter’s drawing of the family showing Beth looking sad and grumpy. Beth prided herself on being bright and bubbly to the outside world. Although no one asked if she was alright, she was not sure she would have said anything anyway.
Beth believes that despite being good at hiding what was happening, the signs were there for others too. She worked at the local hospital and Peter would call eight or nine times during her shift and no one questioned this. Even after she left the relationship, he would visit her at work and stand at the counter talking to her for hours at a time. Beth wished the nursing supervisor or emergency department doctor had told Peter to leave as she was trying work, but the behaviour was ignored, leaving her to deal with it alone. She felt it was safer to just let him talk. When going through court proceedings, her employer said that she’d taken too much time off work (utilising family violence leave) and that she was not welcome to apply for any other leave. Beth does not believe the hospital had any organisational approach to identifying and responding to family violence.
The only institution that said anything was the university, after she went back to study. When she was struggling to complete her assignments, one lecturer asked her about what was going on at home and referred her to the university psychologist. Another lecturer saw the signs, as they were a victim survivor themselves. This was the first time someone told her that she needed to make sure she was safe. The lightbulb moment for her was when she was tasked with writing an essay on the mental health impacts of family violence. She finally comprehended that she was experiencing abuse. This along with the realisation of the impact it was having on her kids was the catalyst for her to finally leave the relationship.
Source: Family Violence Reform Implementation Monitor, based on a direct victim survivor account.
Implementation challenges
A number of implementation challenges were raised that will need to be considered in the ongoing implementation effort
As outlined in Section 1, concerted efforts have been made to build the capability of universal services, however some stakeholders described their experiences of practical, financial and cultural barriers to universal services consistently and effectively identifying and responding to family violence.
Successful MARAM alignment requires a dedicated effort
A clear theme that emerged from our consultations was that a dedicated effort within each service is required to enable effective MARAM implementation, but that this is easier to achieve in some settings than in others. For example, as the Victorian Council for Social Service stated, a large hospital has a far greater capacity to engage than an early childhood centre due to its size, budget and workforce profile.
“Recently diagnosed with breast cancer I have been through the medical system a lot…and unfortunately the same response to my disclosure [of past abuse] every time…no response at all…or maybe a “Oh I’m sorry” and then lets pretend like she didn’t just say that… or I didn’t just hear that…sadly this has been the normal for me…and I imagine if it’s happening to me it’s most definitely happening to others and this does not encourage victim survivors to speak up.”
- Sharon, victim survivor
Two examples from our consultations stood out as being highly effective in their MARAM implementation: Goulburn Valley Health (see Box 1) and cohealth (see Box 2). Both services emphasised the importance of having a dedicated resource within their organisation to drive real change, with Goulburn Valley Health suggesting that family violence roles should be funded for every hospital across the state, and cohealth suggesting that there should be consultants out in the sector to actively support implementation. Indeed, Goulburn Valley Health is considering creating and internally funding a permanent family violence role to lead MARAM alignment work, but not all services have the capacity to do this. Similarly, Early Childhood Australia suggested a family support worker located at each centre or at least attached to a group of centres would greatly support MARAM implementation in the early childhood sector [relates to action 10].
One regional Principal Strategic Advisor noted that there appeared to be an assumption that she and her counterparts across the state could work directly with services to take them through their roles and responsibilities. While some of this work can occur, there can be hundreds of prescribed agencies within a region, and it would be impossible to provide the required level of support to every one of them. We suggest that as part of the planning for the next phase of implementation, consideration should be given to the types of support required to help prescribed workforces embed MARAM in practice; this may include access to dedicated support within organisations.
Box 1: Good practice example - Goulburn Valley Health
Goulburn Valley Health is one of the larger regional hospitals to be funded under the Strengthening Hospital Responses to Family Violence (SHRFV) initiative, with approximately 3,000 staff across multiple sites.
Goulburn Valley Health credits the success of their MARAM alignment to the SHRFV initiative, which included dedicated hospital-specific funding and resources, having a highly engaged and committed executive team (which is briefed on progress every month), and a dedicated trauma-informed services department (believed to be unique to this service), representing a clear location for the leadership of this work.
The team includes a project officer who has mapped all staff roles within the hospital according to MARAM responsibilities to identify gaps in family violence knowledge and skill. The service started aligning to MARAM in August 2020 – including alignment of policies, processes and procedures – and expects to be able to demonstrate MARAM alignment by June 2022.
The service also recognises that staff may have their own experiences of family violence and may need support. In response, they have ‘workplace support’ training aimed at managers and a ‘Family violence support for employees’ procedure. The service representatives we met with also acknowledged there was room for improvement in how they provided ongoing supervision and support to staff who were supporting patients experiencing family violence.
Source: Family Violence Reform Implementation Monitor, based on information provided by Goulburn Valley Health.
Box 2: Good practice example - cohealth
cohealth is a community health organisation delivering services across the northern and western suburbs of Melbourne, with approximately 1,300 staff across its locations.
cohealth has implemented MARAM throughout the service, including customised training (covering topics of relevance to the service such as family violence in the context of same-sex relationships, culturally diverse communities, refugee communities and male victims). It also runs monthly information sessions relating to MARAM, providing an opportunity for staff to ask questions and consult around particular case examples.
cohealth emphasised the importance of its executive being on board, tailored sector-appropriate resources and, importantly, the dedicated consultant it hired using its own funds to lead the change management process and provide workforce support.
Source: Family Violence Reform Implementation Monitor, based on information provided by cohealth.
Reform fatigue and time challenges for multiple workforces
Reform and training fatigue, particularly in the pressure of the ever-changing pandemic environment, was raised repeatedly during our consultations. For example, 84 per cent of hospitals and health services participating in the SAFE audit reported that staff turnover and education fatigue was a key challenge for the sustainability of family violence response achievements in their service.1 Lack of time was the most frequently cited barrier to accessing training and development, based on responses from selected universal services staff responding to the 2019–20 Census of Workforces that Intersect with Family Violence.2
Exacerbating this, in many cases, was a perceived lack of time to participate in training and engage in family violence information sharing, particularly for staff who are casual or all client-facing, including:
- nurses whose working hours are all clinical
- early childhood educators who have minimal time ‘off the floor’
- GPs who are generally operating within small businesses and can’t bill for the work
- rural and remote hospitals relying on locums and travel nurses.
“There is no doubt that frontline workers are missing signs of family violence. At least some of the reason for this is related to time limitations.”
- Lily, victim survivor
The early childhood sector was repeatedly raised as a sector that faced significant MARAM implementation challenges due to a casualised workforce, workforce shortages and high turnover, meaning supporting staff to access training was difficult. We understand that this workforce was one of the few funded for backfill to allow staff to access training, but work is required to improve awareness of this option.
As phase 2 implementation continues, ways to incentivise these diverse and time-poor workforces to engage in training, build their family violence capability and see the inherent value in these activities need to be actively considered [relates to action 10].
The time challenges extend beyond training and capability building, though, with many stakeholders indicating that the time taken for information sharing under the Family Violence Information Sharing Scheme, which can be a key element in identifying family violence, was considerable. We understand that the five-year review of MARAM, which is scheduled to occur during 2022, will further investigate the administrative burden of the scheme on services.
Cultural challenges for the education sector
Early childhood services and schools have a very important role to play in identifying family violence because this sector regularly interacts with families, in some cases over many years. However, because of the close relationships that are formed with families, we understand that this can sometimes lead to a reluctance to raise concerns unless the child is very clearly affected by abuse. The reasons given include that they:
- don’t want to damage the relationship or create awkwardness
- are worried they’ll create problems for the family
- don’t know how to have the conversation.
“I definitely do think frontline workers are missing signs of family violence. I’m not sure if this is because they don’t receive enough training in the area of spotting signs … whether they’re too afraid … because if they do acknowledge they think something is wrong they’re then faced with the dilemma of how to deal with it … and maybe it’s all a bit too hard … or confronting.”
- Sharon, victim survivor
Addressing this reluctance will require a cultural shift, supported by practical guidance around how to have these conversations.
Transitions between kindergarten and primary school, and primary to secondary school, were raised as another area where there was a tendency for kindergarten and grade 6 teachers to avoid including any information about family violence in writing, meaning there is the potential for much of this information to be lost [relates to action 8]. Some schools proactively reach out to each child’s kindergarten or primary school, as appropriate, to gather contextual information about the child and their family situation, but this does not happen consistently. There is an opportunity to place more structure around these transitions to ensure information about family violence risk is consistently communicated to ensure ongoing support for the child and any adult victim survivors.
Funding was a common frustration
Certainty of funding was raised most strongly by the hospital and primary health sectors [relates to action 1].
Hospitals indicated that government investment in the SHRFV initiative, while announced for multiple years, had to be confirmed year to year, and that the uncertainty and late notice of funding allocations for the coming year posed a real implementation risk because staff will look for positions elsewhere. Indeed, some services had lost staff while waiting for confirmation of further funding, resulting in knowledge and expertise being lost and reform momentum being stalled.
While we understand that some uncertainty may be unavoidable, decisions about funding held in contingency (based on performance measures) should be communicated as early as possible – and certainly well in advance of the end of the financial year – to ensure critical staff who are leading this work and who are on contracts are not lost due to late funding confirmation.
Furthermore, to embed and achieve the intended outcomes of the reforms, a longer term commitment to staff capability development – likely beyond the remaining three years of funding – is required. Year-to-year funding is highly problematic, and ideally there should be a realistic assessment of time needed to embed family violence capabilities in practice, and dedicated resources should be confirmed for this whole period. This is particularly important now that the MARAM perpetrator practice guidance is (partly) available, as services will need to begin building capability around working with perpetrators when for many this is an entirely new area of practice.
GPs are another group where major funding issues have been raised. Anecdotally, while GPs are not prescribed under MARAM, most want to improve their ability to identify and respond to family violence to support better outcomes for their patients. However, a major barrier is that the primary health sector is largely made up of small businesses, with billing based on 15-minute Medicare items. There are currently no family violence–related Medicare items, meaning that any extra time a doctor spends collaborating with other services, exploring referral pathways and sharing information is done outside of the standard consultation time, and is therefore unpaid activity.
The draft National Plan to End Violence against Women and Children 2022–2032 states that ‘health service providers such as general practitioners … need to be supported through resources, time and education to identify and respond to family, domestic and sexual violence’ [relates to action 2]. The GP may be one of the few professionals in touch with all members of the family, and we suggest that the national plan may provide an opportunity for Victoria to advocate for creating Medicare items relating to family violence to better account for the time taken to consult effectively with victim survivors (including children) and perpetrators and to respond appropriately. The creation of such items would also help with monitoring the volume and frequency of family violence work for GPs.
Existing Medicare items for chronic disease management and mental health treatment could provide some guidance for creating any future family violence items, including tying access to higher fee items to the completion of training. For example, ‘all GPs are able to access the GP Mental Health Treatment items. However, GPs who have not completed Mental Health Skills Training as accredited by the General Practice Mental Health Standards Collaboration (GPMHSC) will not be able to access higher schedule fee items.’ Given the relatively high rates of disclosure to GPs, it is vital that they be supported to perform this identification and response role.
Endnotes
- The Royal Women’s Hospital and the University of Melbourne (2021): The System Audit Family Violence Evaluation (SAFE) Project, Final Report, p. 5.
- We only considered results for the following workforces: schools, maternal and child health, early childhood, public health services and community health services.
Additional barriers for certain cohorts
Certain cohorts face additional barriers to having family violence identified by universal services
Even where clear signs exist, there are barriers to family violence being identified and raised by universal services, such as a lack of time or confidence. But for some groups, there are additional barriers to having their experience identified.
“Workers need to be open-minded, non-judgemental and provide a welcoming space for discussion to occur; they need to be educated in trauma-informed practice. Not everyone is ready to disclose family violence; some don’t realise it’s happening, others fear systematic interventions and have concerns of their children being taken away. No one wants to be judged for putting up with poor behaviours or their choice to stay in an unhealthy relationship.”
- Ilona, victim survivor
Barriers for diverse communities come up in every area of our monitoring, and although there is often good guidance and training in place around the needs of different groups, putting this guidance into practice is often the challenge. The following cohorts emerged as groups where universal services may be less likely to ask about family violence and/or individuals were less likely to disclose family violence.
This is not intended to be an exhaustive list, nor a comprehensive analysis of the challenges for each group, but rather a snapshot of some of the challenges, and an opportunity to highlight the complexity of supporting universal services to identify family violence for a range of groups within the community:
- Rural/regional – identification of family violence by universal services in smaller communities has been raised as a challenge. We were told about one location where 20 per cent of the community works at the local hospital, leaving victim survivors very reluctant to disclose family violence because they often know the person who is looking after them. Similarly, school staff may have long-standing or family-like relationships with perpetrators, which may impact on victim survivor confidence in disclosing and may result in risk escalation.
- Older people – a very high proportion of elder abuse is perpetrated by family members (and it is often psychological and financial in nature). However, Seniors Rights Victoria explained that health professionals often unknowingly collude with the perpetrator by discussing decisions relating to the older person with them. Groups advocating for seniors explained that older people are often reluctant to disclose family violence directed at them because they don’t want to get their child or grandchild, who are often the ones perpetrating the abuse, in trouble; they want to get them help.
- LGBTIQ+ communities – services working with LGBTIQ+ communities explained that family violence may not even be considered a possibility for a same-sex couple, with signs of abuse sometimes brushed off as family conflict, despite rates of family violence being similar to those for the broader community. The Rainbow Door described an example where a young person called the service after being locked in their room to keep them away from their same-sex partner, only to have it brushed off by some services as a ‘parenting matter’. Thorne Harbour Health also explained that there is often a reluctance to disclose unless there are very clear cues that it is a safe place to do so (such as rainbow flags and signs about family violence in a GP’s office).
- Migrant and refugee – communication barriers and insufficient access to interpreters can mean victim survivors with limited English language skills are less likely to be able to communicate about their family violence situation when engaging with universal services.
- Aboriginal women – due to experiences of intergenerational, systemic racism and a fear of losing children through the involvement of the child protection system, Aboriginal women, children and communities may be particularly reluctant to disclose abuse.
- People with a disability – as noted by the Royal Commission, despite facing a higher risk of experiencing family violence than people without disabilities, victim survivors with disabilities may fear reporting family violence because they don’t think they will be believed, they may lose support (which is compounded in situations where the victim survivor is dependent on the perpetrator for care or other forms of support) or they may have children removed from their care. Similarly, people with disabilities that affect their communication may have trouble conveying their experiences of abuse, and furthermore they may be aware that they are less likely to be regarded as competent or believable witnesses.
- More generally, where the victim survivor doesn’t fit the stereotype, signs of family violence may be missed. Our 2021 report, Accurate Identification of the Predominant Aggressor highlighted the fact that many victim survivors are misidentified as perpetrators due to misconceptions by some professionals about how a victim survivor should look and behave. Similarly, stakeholders shared the following examples:
- A mother of school-aged children who presents with ‘difficult’ behaviour may be seen as a problem and never be considered a possible victim survivor.
- A student displaying challenging behaviours and getting into fights may be punished with detention rather than receiving support.
- Well-educated parents with a higher socioeconomic status may be assumed to be unlikely to be experiencing family violence, and signs of abuse may be disregarded.
- Victim survivors experiencing non-physical forms of family violence may go unnoticed if staff do not have a comprehensive understanding of the signs of these types of family violence.
“Frontline workers need to be aware of behaviours that may make the person or persons experiencing family violence come off as the ‘hard to deal with’.”
- Kelly, victim survivor
“The things I find that are missed is the belief in the story, and the experiences and the walls that are put up by workers when victim survivors present in a way that doesn’t suit the worker’s ideal of how family violence victim survivors should act, feel or respond.”
- Kelly, victim survivor
Further, people with a range of these characteristics can experience overlapping forms of discrimination and marginalisation, and experience further disadvantage in having their family violence identified.
As a representative from the Royal Women’s Hospital told us, intersectionality adds a level of complexity that needs sustained effort and focus. Such matters are included in the MARAM Framework, but as has previously been discussed, many workforces are not engaging with the full suite of MARAM guidance. There needs to be a continued focus through training, guidance and ongoing support for workforces on challenging biases and stereotypes and improving their ability to identify family violence in all its forms and for all cohorts.
“I got expelled in Year 8 with no support. No one helped me find other education options that were suited to my style of learning or to find what I needed. I was seen and treated as a disruption and troublemaker instead of a child trying to ask for help. I was experiencing family violence, in and out of homelessness and a recent sexual assault experience. I wasn’t in a headspace to go to school. It didn’t seem important compared to everything else going on in my life, I didn’t care. I felt like I didn’t matter to the teachers at school. I came to school with self-harm scars that were still bleeding, and they just sent me home with no follow-up. I just felt I was a problem and got punished for things out of my control. I got detentions for not wearing the right uniform and coming to school late. I got suspended for having mental ill-health and told off for showing up late. Not once did someone sit down to just talk and find out what was going on for me.”
- Eliza, victim survivor
Access to services
There is variability in access to services after family violence has been identified
The ability of universal services to identify family violence is an essential component of ensuring victim survivors can be supported earlier. However, support services must be there to respond in a timely way. Victim survivors explained to us that once a victim survivor works up the courage to disclose their situation within a universal service, a lack of corresponding support can be a real disincentive to seek support in the future.
Across all workforces, there seemed to be a clear understanding of what should happen when someone presents in immediate crisis: contact is made with Victoria Police and Safe Steps and, where relevant, a mandatory report to child protection services is made. However, the response for non-crisis situations is less clearly defined, and services can be less readily available.
Many of the matters discussed in this section will be explored in further detail through another monitoring topic later this year when we explore the support available to assist victim survivors in their journey towards recovery.
Specialist family violence services and other therapeutic services
Safe Steps and The Orange Door, where available within a local area, are often listed as the places to call for specialist family violence support for a victim survivor. Safe Steps’ 2020–21 annual report revealed an increase in inbound monthly calls from 5,948 in July 2020 to 9,023 in June 2021, which includes calls from professionals seeking guidance on how to respond to a client. This increase in third-party calls affects the ability of victim survivors seeking immediate support to get through because there is only one line.
Family Safety Victoria has monitored data on referrals from universal services into The Orange Door, and advise that there have not been any manageable demand signals since the phase 2 MARAM commencement. Under The Orange Door service model, every person referred to The Orange Door receives an initial assessment from which they are assigned a priority rating based on risk and need. Those cases that receive a higher priority rating are assigned to a practitioner before those that are assessed as being at lower risk. Many stakeholders we met with, however, indicated that they did not understand the criteria for a case being ‘accepted’ by The Orange Door and felt that access seemed to vary according to demand and capability across sites. However, those we spoke to reflected experiences where victim survivors are referred to The Orange Door but ultimately do not meet the threshold for support, leaving them feeling discouraged and leaving the referring service feeling that the referral did not help.
“Currently, victims of violence are often asked what they need and then told they ‘don’t fit the criteria’, or there are ‘lengthy waiting lists’ or that their case is ‘not a priority’ often because it does not involve physical violence.”
- Lily, victim survivor
We suggest there is a need for clearer communication about how prioritisation of cases at The Orange Door works, clearer criteria for referral to case management, and clearer pathways to other supports to ensure victim survivors and referring services have realistic expectations.
There are also known issues around wait times for therapeutic services more broadly. cohealth explained that there are long waitlists for family violence counselling and that they reluctantly closed their waitlist after it reached 12 months during the height of the COVID-19 pandemic. They also indicated that other agencies were forced to stop accepting new clients or to limit eligibility criteria to manage high demand.
Our 2020 monitoring report described the lack of services for children experiencing family violence as a key issue. The Centre for Excellence in Child and Family Welfare and the Department of Education and Training agreed that in some cases there is a lack of referral options (for example, family violence services designed specifically for children and young people, or services for adolescents using violence against family members or intimate partners), and that wait times are a major access barrier for the therapeutic services that do exist. The Department of Education and Training also noted that schools require parental consent to arrange for a child to participate in a therapeutic service, so if the family is not engaged or the perpetrator won’t agree, the support that can be provided is limited.
Service model for universal services’ ongoing support for victim survivors
Where a patient or student does not wish to access family violence services, where waitlists are preventing timely access to services, or where there are other barriers to seeking support, universal services have an ongoing connection with the victim survivor, and therefore an ongoing opportunity to provide support. Family Safety Victoria indicated that the ongoing support of a trusted professional (such as a GP) is sometimes the most suitable response for the victim survivor.
Some hospitals are already doing early intervention work with victim survivors, including safety planning and support from a social worker.
Director of the Safer Families Centre, Kelsey Hegarty, explained to us that while there is some hesitancy from the family violence specialist sector about GPs doing ongoing safety work with victim survivors, many victim survivors do not take up referrals to specialist family violence services. So, it is extremely important for GPs to not just identify family violence and initiate referrals, but to also provide an appropriate trauma-informed response as part of the ongoing doctor–patient relationship, which may span months or even years.
“Frontline workers in universal services are missing addressing the fact of the long effects family violence has on victim survivors and are responding from a crisis response model and not enough support post crisis.”
- Ilona, victim survivor
In the maternal and child health sector, the MABELS program – a Health Justice Partnership in one region – was established to ‘provide an early intervention response to family violence within the Maternal and Child Health … context by improving the responses of [maternal and child health], legal, family violence and support services in a co-ordinated and integrated manner’. The program is both supporting victim survivors to access support earlier than they otherwise would have and supporting maternal and child health services to better identify and respond to family violence.
The Victorian Principals Association said that, ideally, student support services, such as social workers and psychologists, in each area would provide ongoing support to students in the school context, in partnership with any relevant external services. However, student support services are not consistently available across the state. For example, it is more difficult to fill these positions in regional and remote areas.
PROTECT guidance includes Four Critical Actions for Schools in responding to incidents, disclosures and suspicions of child abuse. Action 4 is to ‘provide ongoing support’ to students affected by abuse. This ongoing support must include developing and implementing a student support plan, regular communication between relevant parties and ongoing monitoring of the student’s wellbeing.
We suggest there is scope to be more specific about the types of support children and young people who are victim survivors may need in order to thrive in the school environment (see Table 5 and Box 3 for examples), and that this advice could be co-designed with young people with lived experience (this is also identified in our Reform Governance report).
Principals would likely welcome this advice: of 600 principals responding to the 2021 Term 3 Principals Survey, many requested further development of family violence resources relating to:
- help with planning support for affected students (372 responses)
- support for addressing safety issues for affected students (332 responses).
Similarly, all sectors should have guidance about what providing ongoing support for victim survivors within their services could look like, and high-level guidance could be provided within the MARAM suite of resources [relates to action 7].
Table 5: Examples of practical actions schools can take to support students who are victim survivors of family violence, as suggested by Berry Street’s team of Lived Experience Consultants
| Allow time to check in individually and chat about how things are going |
| Regularly provide breakfast in the mornings |
| Have a freezer stocked with spare lunches and/or provide canteen vouchers |
| Have a laundry to wash and dry clothes if required, and have spare clothes, socks and shoes available |
| Allow for extensions on assignment due dates, and for assignments to be changed if they include triggering content |
| Make allowances for students to be able to leave the classroom and go outside if needed |
| Understand that, due to their circumstances, students may miss classes or struggle to arrive on time – don’t punish them for this |
| Have dedicated family violence experts within schools |
Source: Y-Change Lived Experience Consultants - Berry Street.
“With schools or bigger universal services there should be a lived experience advocate or trained professional hired for advice or be able to consult or approach families and children about family violence.”
- Kelly, victim survivor
Box 3: Ideal school response to a young person experiencing family violence - a young person's perspective
It is known to the school and teachers that Lenny is experiencing family violence at home. An appropriate and immediate response is taken, and Lenny is receiving the supports they need both in and outside of school. The school and staff are also receiving support from a specialist family violence service to ensure the most appropriate care is provided.
- Lenny has a care plan with the school and is an active part of the decisions that are being made. Lenny is being supported and spoken with in a trauma-informed and child-friendly way, and any revisions to the care plan are made alongside Lenny.
- Lenny is actively involved in their care team meetings in a way that is accessible and safe to them. During these meetings, a safety plan is discussed and documented with Lenny about who the safe people are to pick them up from school and how they will manage the situation if an unsafe person arrives to pick them up from school.
- Lenny can become overwhelmed during class and requires support. Lenny’s teacher is fully aware of what supports to give them. They have packed a bag together that discreetly stays in the classroom, and Lenny is welcome to go to their bag when they start to feel overwhelmed. Lenny worked with a support worker to decide what items are in this bag (for example, fidget toys, snacks, vouchers for the school canteen and other items they need).
- If Lenny needs more help, support staff are available to take Lenny and their bag outside to do some grounding activities together.
- Lenny is supported to catch up on their schoolwork in ways that are not disciplinary in nature, that take Lenny’s concentration and energy levels into account, and that understand Lenny’s capacity limitations while going through a difficult time.
- Peer support is offered to Lenny either through the school or an external specialist support service.
The peer support person also receives regular supervision support and any additional training they might require for their peer support role within the classroom.
Source: Y-Change Lived Experience Consultants - Berry Street.
Creating a clearer service system for both victim survivors and services
We suggest many of the issues above could be addressed by a clearer service model that describes service pathways for people with different risk levels and in different circumstances, with clear access criteria for each. We understand there are some practical realities to this, such as heightened demand leading to services having to create stricter criteria. However, a documented map of how the service system should work would be a good starting point [relates to action 3].
One of the victim survivors we met with shared her experience where she had her family violence identified within universal services but then faced major barriers when trying to access support because the perpetrator lived overseas (see Anna’s experience below). She described trying to navigate the family violence and related service systems herself as overwhelming. Another victim survivor had a similar experience, and wished she’d been given a sheet of paper outlining contact details for the various support services available and a clear description of what each service does. This ‘low risk’ cohort, which may not meet the threshold for specialist services, would benefit from an overview of the services they may need to access to ensure they are not forced to blindly navigate the service system. These experiences also suggest that the support for victim survivors in navigating the service system envisioned in Victoria’s 10-year family violence plan has not yet been realised. The plan stated:
Victim survivors will not have to navigate the complex legal and community services systems by themselves. Service navigators will be highly skilled specialist workers that will have the flexibility and capacity to support people from crisis through to recovery, and ensure they are supported in a simple, timely and coordinated way that works for them.
“Navigating services post-separation was described to me many years ago as ‘jumping into a safety net full of holes’. This remains true in 2022, where services are often stretched beyond capacity. Circular referrals are a real thing. Victims are referred to a service, but when they call, they are provided with a number for a different service, and another and another. Sometimes they are referred right back to the original service. Victims of violence frequently express being ‘exhausted’ from navigating ‘systems’ and getting nowhere.”
- Lily, victim survivor
Anna's experience
Anna met Ben overseas and the relationship started off like a romantic comedy. But once she found out she was pregnant, everything changed. Ben became very controlling, restricting her movement out of the house and even withholding food and water from her. After about a month, she managed to escape back to Australia, her home country, although he continued to abuse her via her phone, including threatening to take the baby away from her once it was born. She had no idea what her rights were, especially with the added complexity of him living overseas.
Anna never thought of this behaviour as family violence; she just thought she was in a bad relationship. It wasn’t until she confided to her midwife about her situation that she came to see it as family violence. The midwives in the maternity ward were great and put strategies in place to make her feel safe, particularly as she knew Ben was coming to Australia around this time. They also linked Anna up with a social worker, who visited her at the hospital.
Because Ben lives overseas, Anna has struggled to get the support she needs. Anna was referred to The Orange Door, but it was deemed there was no immediate risk, so they couldn’t help her. She also put together a safety plan with Safe Steps for if Ben entered the country, but she never received a copy of this plan, and couldn’t remember most of what was discussed. Anna reached out to Victoria Police and found them unhelpful; however, she has since found out that there are specialist units responding to family violence, but she felt like these units were kept secret. She has also received conflicting advice about applying for a family violence intervention order, with some saying it is not possible because it is unable to be served to Ben because he is living overseas. Anna worries that because there are no legal orders in place, if they end up going to court, she may not be believed.
After that first identification point, Anna wishes that she had been offered early legal advice and had been linked with the appropriate services, who could respond to abuse being perpetrated from outside Australia. This would have made her feel protected and safe.
Source: Family Violence Reform Implementation Monitor, based on a direct victim survivor account.
Secondary consultations
A clear model for secondary consultations would improve coordination and consistency
Responsibility 5 of the MARAM Framework is secondary consultation and referral. Secondary consultation can occur with a range of services, but for this report, our focus is on universal services reaching out to specialist family violence services to seek expert advice.
While we understand that seeking secondary consultation is an expected part of good, collaborative practice in the MARAM Framework, our consultations suggested there is a lack of structure, guidance and monitoring around secondary consultations at the system level. This includes a lack of specific guidance about what should happen where a specialist family violence service identifies a client as high risk through a secondary consultation.
Family Safety Victoria explained that secondary consultation models for particular workforces were the responsibility of implementing agencies, and that secondary consultations have not been raised as an issue in bilateral meetings with agencies nor by sector grants groups. We suggest, however, that the matter needs to be discussed with specialist family violence services and peak bodies, The Orange Door locations and family violence regional integration committees to get a better sense of some of the issues and to ensure a consistent and systemic approach to secondary consultations.
Within the MARAM Responsibility 5 practice guide, there is detailed information about why a service might reach out to another service for the purpose of a secondary consultation. It explains that ‘the purpose of secondary consultation with specialist family violence services is to seek support in:
- understanding the level of risk and intersectional needs
- determining actions in line with the assessed level of risk
- determining whether a referral is required for a specialist family violence response’.
The practice guide advises services that The Orange Door, where it exists, is a good point of first contact for a secondary consultation, or otherwise a local specialist family violence service. Family Safety Victoria also advised that the statewide contact points are Safe Steps and the Men’s Referral Service. Beyond this, we are not aware of a specific system-wide model for secondary consultations, and some stakeholders have suggested there should be one.
Increasing demand for secondary consultations
With universal services coming into scope for the rollout of MARAM and the information sharing schemes, many stakeholders expressed that an increase in secondary consultations with specialist family violence services was to be expected, as universal services build their capability in responding to family violence and their understanding of their new obligations. For example, during phase 1 of the reform rollout, EACH, a nation-wide provider of a range of social and health services, noted that ‘in one region secondary consultation requests from EACH to the regional specialist agency increased from 30 during the 2018/2019 financial year, to over 130 requests in the 2019/2020 financial year’.
As the Central Highlands Integrated Family Violence Committee noted in its 2020 submission to the Monitor:
In the context of significant difficulties with the roll-out and engagement of training, newly prescribed organisations are likely to turn to secondary consultation – as required by their MARAM practice guidance – to support them in understanding a family violence situation, assessing it and managing the risk. There is also likely to be significant overestimation of risk in some circumstances due to risk aversion amongst a very large workforce, leading to cases being referred for comprehensive response unnecessarily.
The Western Integrated Family Violence Committee has raised a similar issue:
Secondary consultation is a vital component of the collaborative practice outlined under MARAM, however there are substantial barriers to accessing secondary consultation within the western metropolitan region … the demand for secondary consultation will only increase when phase 2 organisations are prescribed under MARAM and the Information Sharing Schemes.
Anecdotally, incoming secondary consultations have been increasing for many specialist services and sectors such as Drummond Street Services, Safe Steps and specialist sexual assault services. The Rainbow Door and Seniors Rights Victoria noted that they also receive a large number of secondary consultations and are not adequately funded to do this properly.
Several family violence regional integration committees we met with were leading projects of various sizes to quantify demand for secondary consultations in their regions because it is not something that is otherwise measured. Safe and Equal is doing similar work, but a statewide view of demand and impact will be important to determine whether there are any widespread funding or service delivery implications. Given the critical role secondary consultation plays in the family violence system, we suggest it will be essential to quantify this demand and monitor it in an ongoing way across the system, including tracking where the requests are coming from and time spent on secondary consultations [relates to action 5]. This will assist in designing the most effective model(s) for secondary consultation and could inform training and capability building approaches for different workforces.
There has been some progress in tracking secondary consultations in recent years. Family Safety Victoria has advised that, since 2020, the case management platform used by specialist family violence services has included an option to record secondary consultations. A March 2022 enhancement to The Orange Door’s client relationship management system now also allows practitioners to record secondary consultations, including the time taken.
Many stakeholders raised the lack of specific and sustainable funding for secondary consultations as a key issue. We understand that Case Management Program Requirements for Specialist Family Violence Services, released in December 2021, describe secondary consultations as an integral part of case management functions and include requirements that agencies have processes in place to respond to and seek secondary consultations. However, there are no service delivery targets connected to this, which results in secondary consultations being invisible within the current funding structure. It also makes it difficult to determine if services receive adequate funding to account for the increase in volume of secondary consultations that is expected as universal services start to identify more family violence. We were advised that the time taken for each consultation can be substantial, with No to Violence and Safe and Equal stating that 45–60 minutes for a secondary consultation would not be unusual; one Principal Strategic Advisor said consultations can be as long as 90 minutes.
While there is no specific performance target for secondary consultations, in the new funding model for specialist family violence services to begin in July 2022, funding explicitly covers secondary consultations and services will be able to count the time spent on secondary consultations towards their overall performance targets.
The role of The Orange Door
The Royal Commission saw a very clear role for The Orange Door in providing secondary consultations to universal services. As part of the introduction of The Orange Door, it was recommended that new advanced family violence practitioners be funded at each site to assist their colleagues with complex cases and to provide ‘secondary consultation to local GPs and health practitioners, schools and other service providers who have clients experiencing or at risk of family violence’. Under this model, ‘there is a defined role of secondary consultation and capability building with non–family violence services’.
These roles do exist as advanced family violence practice leaders across The Orange Door sites (see Table 6), and the responsibility for delivering external secondary consultations is documented in The Orange Door’s operating model as one of many responsibilities (see Box 4). However, Family Safety Victoria has advised that secondary consultations will usually occur directly with The Orange Door practitioners, while practice leaders primarily provide advice and guidance to practitioners. This may be appropriate, but we suggest there needs to be further examination of how secondary consultations are being managed and delivered within The Orange Door model, and that the approach be clearly documented [relates to action 5].
Table 6: Advanced family violence practice leader positions and vacancy rates, January 2022
| Advanced family violence practice leader |
Advanced family violence practice leader (men’s) |
|
|---|---|---|
| Large metro sites ie: Bayside Peninsula Area, North East Melbourne Area, Brimbank Melton* and Western Melbourne Area* |
2 positions | 1 position |
| All other sites | 1 position | 1 position |
| Vacancy rate | 33% | 24% |
*future sites
Source: Department of Families, Fairness and Housing
Box 4: Role of advanced family violence practice leaders at The Orange Door
- Lead clinical practice and jointly manage cases
- Oversee referrals to Risk Assessment and Management Panels (RAMPs)
- Prioritise and approve Central Information Point (CIP) requests
- Clinical advice and decision making in family violence cases where there are different views within The Orange Door team
- Deliver practice leadership and secondary consultation to service providers on family violence beyond The Orange Door, consistent with MARAM Framework responsibilities 5 and 6
- Contribute to case reviews, practice reflection and learning and development to build The Orange Door workforce capacity in family violence, including capacity to address the range of presentations of risk across the community and applying an intersectional lens
- Build baseline family violence navigation capability.
Source: Family Safety Victoria (2019): The Orange Door: Service model, pp. 19–20.
The case for a stronger system model for secondary consultations
As the Victorian Council for Social Service told us, effective system integration and collaboration needs to have a system-level solution. While personal, local relationships can be effective, they do not necessarily lead to sustainable improvement, nor consistent practice across the state.
As a prominent family violence organisation, Safe Steps is often contacted for secondary consultations, and sees itself as a logical contact point for universal services needing specialist advice, particularly after hours given it is a 24-hour service. However, incoming calls – many of which are estimated to be from third parties such as schools, doctors and hospitals – have increased substantially. In developing a model for secondary consultations, the role of Safe Steps needs to be included, and consideration should be given to introducing a separate phoneline for third-party calls from health and education professionals.
Western Integrated Family Violence Committee provided us with its project proposal for ‘embedding family violence secondary consultations in the western metropolitan region’. This document usefully highlights secondary consultation as:
- a mechanism to build family violence knowledge and practice across the service system
- supporting earlier interventions in family violence, thereby reducing harm to victim survivors
- a strategy for mitigating high levels of demand for specialist family violence services by empowering a system response before risk escalates
- supporting MARAM alignment for all prescribed services, fostering family violence knowledge, embedding collaborative practice, and strengthening referral pathways.
It also recognises that realising these outcomes requires adequate guidance and capability building in how to conduct high-quality secondary consultations [relates to action 4]. Local partnerships and strategies are important, but we suggest efforts to improve secondary consultations
need to occur at a higher level and focus on appropriate models for particular workforces – and, where appropriate, for particular geographic areas – to define how the specialist family violence sector, Family Safety Victoria and relevant implementing departments want universal services to engage with the specialist system. Victoria’s family violence regional integration committees will also have an important role, as will Aboriginal Community Controlled Organisations (to ensure a culturally safe response for Aboriginal people).
Ongoing monitoring
Ongoing monitoring of reform progress and impact is essential
Monitoring the impact of MARAM, and the effectiveness of various approaches to its implementation, is critical to inform future planning and effort.
Evaluation
It is positive that evaluations have been planned in some areas. A maternal and child health family violence evaluation will attempt to measure practice change as a result of MARAM and information sharing. The evaluation has been delayed due to significant demand and workforce pressures on the maternal and child health workforce due to the COVID-19 pandemic, but the report is expected to be available in late 2022. An evaluation of MARAM implementation in education settings has also been funded, but has not yet begun.
Hospitals have expressed frustration about evaluation not being built into the funding model for the SHRFV initiative. Representatives from the hospitals leading this initiative explained that there is a strong need for data and evaluation to help this work become business as usual by ensuring there is a documented, evidence-based case for the benefits of the program. For example, according to the Royal Women’s Hospital, there has not been a large increase in referrals to specialist family violence services due to family violence screening occurring in its antenatal service, and this is likely because the hospital is intervening earlier and working directly with some patients. However, due to a lack of evaluation resourcing, SHRFV has no capacity to collect corroborating evidence. Other hospitals, particularly those where social work is not consistently available, have indicated that they have seen an increase in referrals to specialist family violence services.
The SAFE audit conducted as a one-off project across multiple health services and hospitals with the support of philanthropic funding has provided a good snapshot of how well hospitals are set up to identify and respond to family violence. The SAFE Project report1 recommended:
- regular review of demand associated with family violence work
- regular auditing including SAFE Tool implementation.
However, doing this kind of auditing requires ongoing resourcing, as we were advised that the 50-file audit that is required takes approximately three weeks for one person. Some hospitals are initiating their own studies of the effectiveness of their approach to SHRFV implementation (for example, see Box 5), but these rely on clinician-reported knowledge and confidence.
Box 5: Evaluation activity at the Royal Melbourne Hospital
As part of its implementation of the SHRFV initiative, the Royal Melbourne Hospital implemented an evidence-based and in-depth training framework for its 6,000+ workforce, in conjunction with a clinical champions network (called the Family Safety Advocates Network). This was a network of staff who received more than nine hours of family violence–related training and consisted of health professionals throughout the hospital.
A study evaluated the clinical champions model in allied health staff. The study found that the model resulted in statistically significant and sustained improvements in levels of self-reported family violence knowledge, confidence and frequency of screening, when combined with a community of practice.
The hospital is also assessing the three-year impact of SHRFV through a 2020 evaluation (yet to be published). The evaluation found that, compared with the baseline knowledge of all staff, as assessed in 2017, there were statistically significant increases in knowledge, confidence levels and how often family violence screening was occurring. There were also self-reported improvements in staff knowledge about key indicators of violence and in their ability to ask about and respond to disclosures of family violence.
Source: Family Violence Reform Implementation Monitor, based on information provided by the Royal Melbourne Hospital.
System-level monitoring
Governance groups and bilateral meetings between Family Safety Victoria and departments supporting prescribed sectors provide an important communication line for raising implementation issues, and we suggest that such feedback be actively sought from frontline workforces [relates to action 12].
Data and evidence are also required. Family Safety Victoria worked with Cube Group in 2019 to develop a MARAM monitoring evaluation plan and framework. These highlighted existing mechanisms for data collection, such as those listed in Table 7, each with its own challenges and opportunities. The monitoring plan also proposed a series of measures that Family Safety Victoria hoped to capture via individual services, including those outlined below, but we are not aware of whether data against these measures could be obtained:
- number of referrals made to other framework organisations, by type of framework organisation
- number of referrals received by other framework organisations, by type of framework organisation
- number of requests for or provision of secondary consultations related to family violence
- number of referrals made and received for clients from Aboriginal communities, diverse communities and at-risk age cohorts
- number of victim survivors identified by universal or non-specialist services who are referred to appropriate services.
Table 7: Ongoing monitoring of MARAM implementation – challenges and opportunities associated with using existing data sources
| Existing data sources* | Challenges | Opportunities |
|---|---|---|
| Census of Workforces that Intersect with Family Violence |
According to reporting on the 2019 census, only 1% of the estimated 222,070 workers in broader workforces that intersect with family violence responded to the survey (which includes workforces in scope for this report as well as many others, including police, courts, etc.). | The 2020 process evaluation of the MARAM reforms suggested using future iterations of the census to determine the level of awareness, understanding and use of the MARAM Framework. |
| Post-training surveys | Preliminary findings from the evaluation of the Strengthening the Foundations Rolling Action Plan suggest that objective measures of learning are rarely used, undermining the veracity of some evaluations. | The limitations of these surveys need to be acknowledged and results coupled with more objective data on the impact on practice. |
| Framework organisations survey |
The survey has only been done once, in April/May 2021, and did not cover phase 2 organisations. Encouraging a strong response rate from universal services will In addition, the survey only captures the perspectives of the most senior staff within each organisation who are responsible for and involved in implementing MARAM in their organisation. |
Results for universal services, particularly broken down by workforce, will provide a good snapshot of MARAM understanding and implementation, indicating things like:
|
| Family violence– related data reported by agencies |
Much of the data reported by implementation agencies seems to focus on training numbers. Again, preliminary findings from the evaluation of the Strengthening the Foundations Rolling Action Plan noted that training numbers are not always connected to workforce planning, therefore the scale of achievement is unclear and the remaining need not quantified. |
We suggest further emphasis be placed on building the capacity of agencies to report on measures that can provide a greater sense of impact. Data on referrals to The Orange Door, including the source, is tracked, and it will be useful to also track incoming secondary consultations through the new data fields recently added to the client relationship management system. |
Source: Family Violence Reform Implementation Monitor, based on information provided by Family Safety Victoria.
* As identified in the MARAM monitoring and evaluation framework.
There are multiple other sources of data, such as surveys (for example, the Department of Education and Training’s principals survey, which includes a range of MARAM and information sharing–related questions) and evaluations. We suggest it is vital that monitoring and evaluation activity be built into ongoing practice wherever possible, and that this data be brought together to form a coherent and meaningful view of MARAM implementation across the system, with an emphasis on impact [relates to action 13].
Ongoing monitoring of MARAM across workforces could focus on answering questions such as:
- What is the family violence identification rate?
- How is practice changing for different workforces? How does it vary across locations? What training have staff done?
- What outcomes are being achieved for victim survivors?
- Where are clients experiencing family violence being referred? Are services meeting demand? Where are there blockages? What support is being provided by universal services in these situations?
- What is the percentage of people who can be appropriately supported without referring onto specialist family violence services?
- What is the frequency of, and time taken for, secondary consultations and information sharing? For example, the regulatory impact statement included a range of assumptions, including an estimated 30 minutes per MARAM response for phase 2 organisations. It will be important to determine whether these estimates are reasonable or require revisiting to inform future planning. It will also be useful to track which sectors are making these requests, what they are requesting and of whom [relates to action 5].
MARAM Maturity Model
A MARAM Maturity Model project is currently underway and will involve developing products such as a maturity matrix against which organisations can plot their progress, a range of resources to support alignment and an improvement cycle (as depicted in Figure 6). As discussed in our Reform Governance report, this work builds on the existing Organisational Embedding Guide, released in 2020. The improvement cycle is expected to operate at two levels: at the program area level, whereby sector maturity is assessed, improvement strategies put into place and then reviewed; and at the individual service level.
Once this model is in place, it has the potential to be a key source of information about the effectiveness of MARAM implementation. How departments will engage with the model, and how they will support prescribed organisations to engage with it, is yet to be determined.
The MARAM Framework is the foundation for a unique and ambitious whole-of-system approach to identifying and managing family violence risk. An ongoing emphasis on monitoring, evaluation and data is required to ensure progress can be accurately monitored, opportunities for improvement can be identified, and the framework can become embedded across the system.
Figure 6: Proposed improvement cycle for the MARAM Maturity Model

Source: Family Safety Victoria
Endnotes
- The Royal Women’s Hospital and the University of Melbourne (2021): The System Audit Family Violence Evaluation (SAFE) Project, Final Report, p. 48.
Family violence services and support
If you are concerned for your safety or that of someone else, please contact the police in your state or territory, or call Triple Zero (000) for emergency assistance.
If you have experienced family violence and need support or assistance, contact:
- National Sexual Assault and Domestic Violence hotline 1800 RESPECT (1800 737 732)
- Safe Steps 24/7 family violence response line 1800 015 188
- Victims of Crime helpline for men experiencing family violence 1800 819 817 (8am-11pm)
- Rainbow Door specialist LGBTIQ+ support, advice and referral line 1800 729 367 (10am–5pm).
If you are concerned about your behaviour and its impact on your family, contact the Men’s Referral Service on 1300 766 491 (8am–9pm).
Victim survivor acknowledgement
We acknowledge the terrible impact of family violence on individuals, families and communities, and the strength and resilience of the children and adults who have, and are still, experiencing family violence.
We pay respects to those who did not survive and to their family members and friends.
Aboriginal acknowledgement
The Victorian Government proudly acknowledges Victorian Aboriginal people as the First Peoples and Traditional Owners and custodians of the land and water on which we rely.
We acknowledge and respect that Aboriginal communities are steeped in traditions and customs built on an incredibly disciplined social and cultural order. This social and cultural order has sustained up to 60,000 years of existence.
We acknowledge the ongoing leadership role of the Aboriginal community in addressing and preventing family violence and join with our First Peoples to eliminate family violence from all communities.
Glossary
| Aboriginal | While acknowledging the diversity of Aboriginal people in Australia, in this document the term ‘Aboriginal’ has been used to refer to all people of Aboriginal and/or Torres Strait Islander descent. |
| Child Information Sharing Scheme | Established in legislation, the scheme provides for sharing of information among authorised organisations to promote child wellbeing or safety, including within (but not limited to) family violence contexts. |
| Collude | Intentional or unintentional collaboration with a perpetrator by reinforcing, excusing, minimising or denying a perpetrator’s violence towards family members. |
| Family Safety Victoria | A division of the Department of Families, Fairness and Housing with dedicated responsibility for delivering key elements of the family violence reform. This includes the Family Violence Information Sharing Scheme, The Orange Door network and the Family Violence Multi-Agency Risk Assessment and Management reforms. |
| Family violence | Any violent, threatening, coercive or controlling behaviour that occurs in current or past familial relationships, including by intimate partners, family members, and/or non-family carers. |
| Family Violence Information Sharing Scheme | Established in legislation, the scheme enables sharing of information between authorised organisations to support the assessment and management of family violence risk. |
| Family Violence Multi-Agency Risk Assessment and Management (MARAM) Framework | A framework to support the identification, assessment and management of family violence risk. A range of organisations are required by law, under the Family Violence Protection Act 2008, to align their practices and policies with MARAM, which replaced the former common risk assessment framework or ‘CRAF’. The MARAM Framework is supported by operational practice guidance and risk identification, screening and assessment tools. |
| Family violence regional integration committees | Local governance partnerships in 14 areas across Victoria bringing together family violence services and other key sectors and services, including child and family services, child protection, mental health services, homelessness services, housing services, courts, police and Indigenous Family Violence Regional Action Groups, to improve the integration of local services that respond to family violence. |
| LGBTIQ+ | An inclusive initialism that refers to lesbian, gay, bisexual, transgender, intersex and queer people. |
| MARAM | See Family Violence Multi-Agency Risk Assessment and Management (MARAM) Framework. |
| Phase 1 | Phase 1 of the information sharing and MARAM reforms began on 27 September 2018, when more than 850 organisations were prescribed to the reforms. More than 35,000 professionals from organisations including those in the specialist family violence sector, including The Orange Door staff, and services in alcohol and other drug, child protection, homelessness, courts, police and corrections, noting that not all were prescribed to all three of the reforms. |
| Phase 2 | Phase 2 of the information sharing and MARAM reforms began on 19 April 2021, when more than 350,000 additional professionals from approximately 8,000 organisations were prescribed to the reforms. This phase comprised mostly of universal services, including health and education services. |
| Prescribed organisation | Organisations that must meet the responsibilities set out under the Multi-Agency Risk Assessment and Management Framework, the Family Violence Information Sharing Scheme and/or the Child Information Sharing Scheme. |
| Principal Strategic Advisor | A key leadership role within the family violence regional integration committees. This role has a strong focus on integration and collaboration of services, driving implementation of the reforms and capacity building of the workforce. |
| PROTECT guidance | Resources developed to support school staff in all Victorian schools to identify and respond to all forms of violence, including child abuse and student sexual offending. |
| Respectful Relationships | A primary prevention education initiative that supports government, Catholic and independent schools and early childhood settings to promote and model respect, positive attitudes and behaviours. The Victorian Curriculum provides the basis for teaching and learning about respectful relationships and identifies the knowledge, skills and understanding for students to be able to engage in respectful relationships. |
| Royal Commission into Family Violence | Established in 2015, the Commission was tasked with finding ways to prevent family violence, improve support for victim survivors and hold perpetrators to account. The Royal Commission provided its report, which included 227 recommendations, to the Victorian Government on 29 March 2016. |
| Secondary consultation | A mechanism by which professionals can seek guidance or advice from specialist services when supporting those impacted by family violence, to determine the appropriate response based on risk and needs. |
| SHRFV | See Strengthening Hospital Responses to Family Violence. |
| Strengthening Hospital Responses to Family Violence | A system-wide model for hospitals to educate and support their staff in identifying and responding to family violence experienced by patients, as part of a whole-of-hospital approach. |
| The Orange Door | A network that is the entry point to women’s and children’s family violence services, services for men who use violence and family services. It undertakes triage to assess and manage risk and connect people to the services they need. |
| Victim survivor | A person who has experienced domestic, family or sexual violence. |
| Victim Survivors’ Advisory Council | Formed in July 2016, the council was established to include people with lived experience of family violence in the service design of the family violence reform. |