
Workforce is a critical part of prevention system architecture, with the ability to achieve outcomes in large part depending on having a skilled, stable workforce in place to deliver the work [relates to action 6].
Who makes up the prevention workforce?
Noting that the prevention capability framework is in the process of being updated, the inaugural version defines the prevention workforce in two parts:
- Prevention practitioners – those who ‘specialise in designing, implementing and monitoring actions to prevent violence against women. [Prevention of violence against women] practitioners must understand the drivers of violence against women and are engaged in activity that focuses on actions to prevent violence before it starts’ (though we understand the workforce prefers the term ‘prevention specialists’).
- Prevention contributors – ‘those who are located within specific sectors or disciplines where participation in [prevention of violence against women] practice may be a part of their role, but is not their primary focus. These practitioners include teachers, health sector staff, sports administrators, local government staff, human resources staff, child and family services staff, evaluators, workforce trainers or communications personnel.’
Many stakeholders found it difficult to define precisely who the primary prevention workforce is, with one commenting that this could change from year to year, depending on where grants are allocated and shifting organisational priorities. Most stakeholders were clear, however, that prevention specialists in women’s health services are the main experts in this space. We understand that the review of the prevention capability framework will look at supporting a clearer definition of the roles within prevention, including that of prevention contributors.
In preparation for the 2019–20 Census of Workforces that Intersect with Family Violence, the size of the primary prevention specialist workforce in Victoria had been estimated to be 352 people; however, there were 517 responses to the primary prevention census survey. The survey findings report outlined possible explanations for this: the population size may have been underestimated or respondents may have mistakenly classified themselves as prevention specialists.
Gender Equity Victoria told us that compared with the response sector, the specialist prevention workforce relies on networks and partnerships to progress its work, and that, for this reason, it is often seen as ‘messy’. Similarly, Women’s Health Victoria explained that there is not a ‘primary prevention service system’ like there is in the family violence response space; rather, there are people in all types of organisations that together constitute the prevention workforce. Indeed, the workforce census results confirm that prevention specialists work across a range of different organisation types and settings (see Figure 12).
While the dispersed nature of the workforce is not necessarily a problem, having an accurate picture of the specialist prevention workforce will be essential for future workforce planning.
Figure 12: Proportion of prevention specialist by organisation type

Workforce strategy
The industry plan recognised the need for a ‘strong pipeline of dedicated, skilled and diverse workers for the specialist family violence and primary prevention sectors’ to ensure the full value of the Victorian Government’s substantial investment into family violence reform can be realised. More recent consultation with the sector around Victoria’s approach to primary prevention reiterated the need for the government to pursue strategies that aim to widen the prevention workforce pipeline.
Initiatives led by the Centre for Workforce Excellence have had the primary prevention workforce in scope. For example:
- The family violence attraction and recruitment campaign includes resources aiming to attract people to the prevention workforce and links to prevention roles included on the jobs portal.
- The Family Violence and Sexual Assault Graduate Program is trialling the inclusion of primary prevention placements, with two graduates taking on primary prevention roles in 2022.
- The Fast Track program (delivered by Safe and Equal) aims in part to fast track the supply of knowledgeable and skilled practitioners able to take up mid-level roles in the primary prevention of violence against women.
We do not have enough information to comment on the effectiveness of these initiatives, but it is well accepted that a dedicated plan for the family violence prevention workforce is required, building on existing work such as the prevention capability framework and the industry plan. The Family Violence Reform Rolling Action Plan 2020–2023 included the following action to be completed by early 2021:
A plan for supporting the current and growing primary prevention workforce is developed in consultation with stakeholders, including ways to engage with broader workforces to help in prevention efforts. This plan will complement the Industry Plan for workforce development.
Behind the scenes during 2020 and 2021, there have been some significant pieces of work completed to map the workforce and prevention infrastructure more broadly, but this has not yet been translated into an agreed plan. The sector is eagerly awaiting the release of this work, with one stakeholder wanting to know what the approach will be before planning for its recent four-year funding allocation for workforce capability building. One opportunity to progress this work is embedding it within the forthcoming second rolling action plan to the industry plan.
Undoubtedly, widening the pipeline and attracting more people to primary prevention roles will be vital as prevention necessarily becomes a growing focus within the reform program to reduce the rate of family violence. This will likely need to be done in tandem with work to clarify the system architecture and theory of change. It must involve Respect Victoria, the Office for Prevention and the Centre for Workforce Excellence, in consultation with the sector.
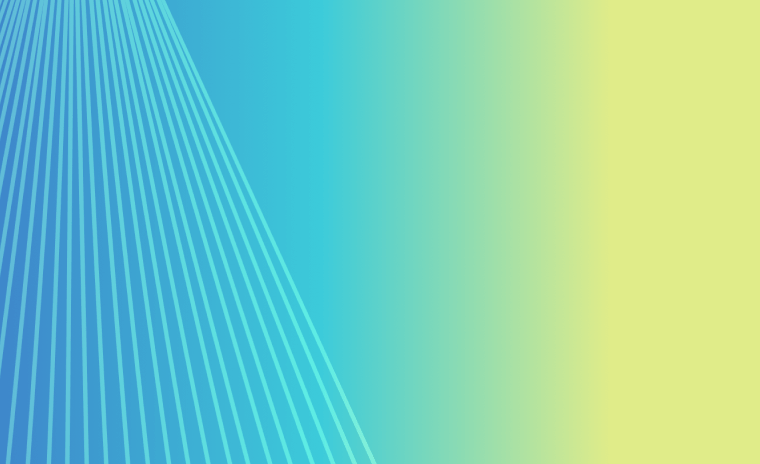
The plan will need to carefully account for the workforce’s professional development needs. Prevention specialists tend to have a high level of education (see Figure 13), but they also vary in their level of confidence to undertake family violence prevention work and are committed to their professional development. For example, the workforce census found that around half (49 per cent) of respondents were extremely or very confident that they had enough training and experience to perform their role effectively (there was a higher level of confidence for specialists in women’s health services: 68 per cent). Thirty-three per cent of respondents said that increased availability/accessibility of training or professional development would help them carry out their role more effectively. And approximately 73 per cent of survey respondents identified one or more areas in which they wanted more training. Consideration of how to build capability in an integrated workforce, such as the workforce within Aboriginal Community Controlled Organisations, which do not include prevention specialists specifically, is also needed.
Figure 13: Education level and areas of study of prevention specialists
More broadly, Safe and Equal suggested there would be value in better articulating primary prevention roles beyond the currently used broad terms of prevention 'specialists' and 'contributors', which are terms that the diverse range of professionals working in prevention may not identify with, so that the workforce strategy, including capacity building, can be more targeted.
As highlighted in our 2020 report, there is a need for a concurrent focus on workforce retention to maximise the long-term impact of attraction and recruitment initiatives. Many stakeholders commented that pay and conditions for primary prevention roles need to be addressed, highlighting issues such as:
- the prevalence of short-term contracts (for example, 1–2 years)
- the low level of remuneration, meaning that some prevention specialists have had to take second jobs in retail to be able to continue this work
- under-funding of prevention work to meet demand, meaning that prevention specialists (such as those in women’s health services and sexual assault services) are sometimes called upon to provide their expertise for free
- funding uncertainty, making the effective delivery of prevention activities and retention of skilled staff more challenging [relates to action 7].
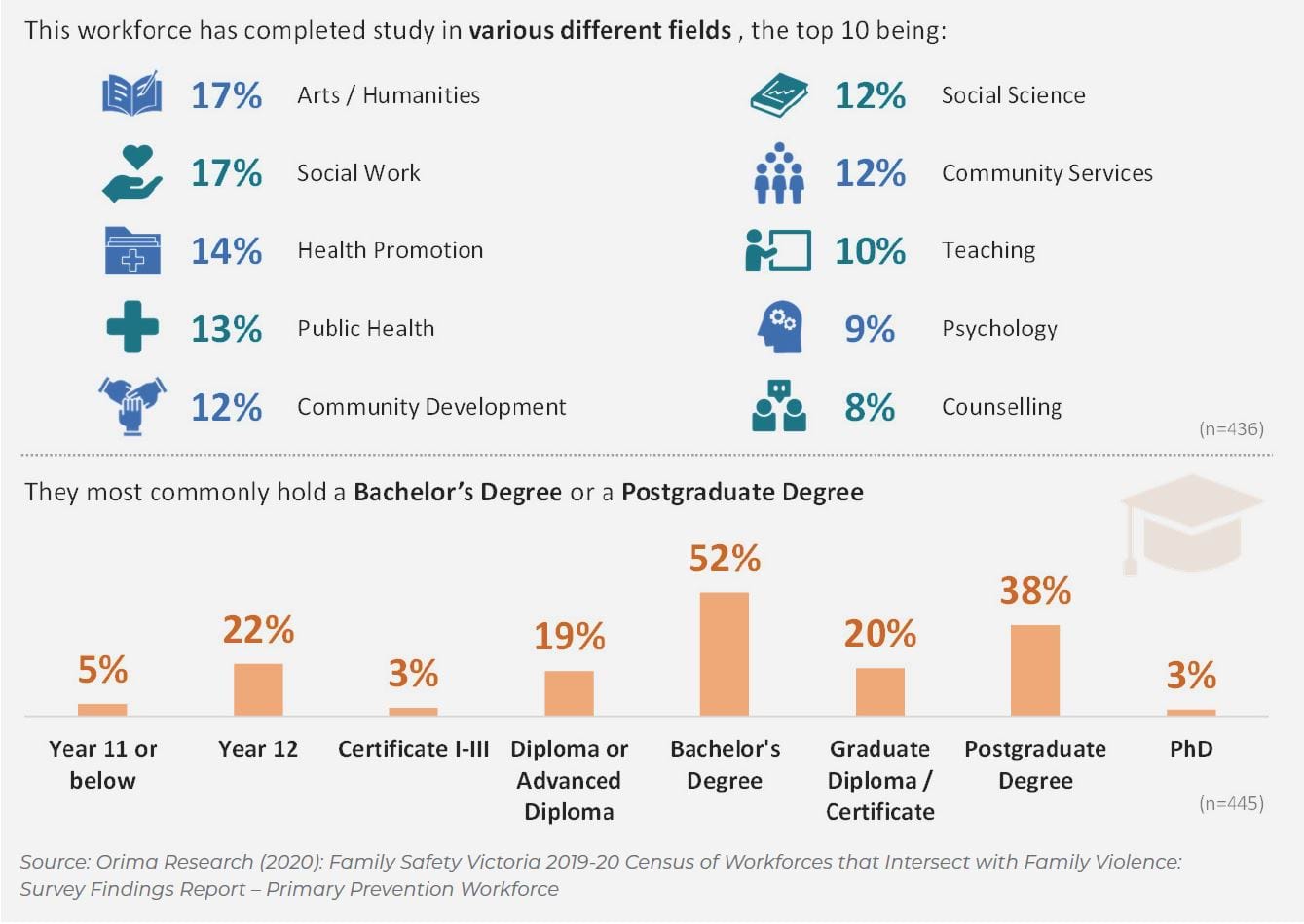
These issues significantly affect retention. Strikingly, the workforce census found that nearly half of all respondents had plans to leave their current role, mostly due to their contract ending (see Figure 14).
Further, despite high levels of satisfaction with their roles and strong intrinsic motivation for the work, of those intending to leave, 41 per cent were planning to go to another role outside primary prevention and 32 per cent were planning to go to another primary prevention role.
According to the workforce census, 85 per cent of the primary prevention specialist workforce is female. One stakeholder made the point that prevention progress in Victoria has been built on the goodwill of women with low-paid and insecure jobs (despite many having university-level health promotion type degrees) – the very factors that contribute to gender inequality and violence against women.
Figure 14: Prevention specialists' plans to leave their current role
To address the retention issues, and to show that this work is truly valued, work to enhance pay and conditions in the prevention sector will be essential. This is particularly important in the context of the obligations created through the Gender Equality Act, which we understand is in some cases seen to be exacerbating existing retention issues in the prevention sector because staff are drawn to more highly paid gender equality jobs in government agencies, universities and local government. Both gender equality and primary prevention workforces are critical and both are leading mutually reinforcing work. The government must work to ensure that pipelines into both workforces are broadened concurrently.
The plan will also need to cover prevention contributors. Safe and Equal explained that universal services are essential in the family violence prevention space – the relatively small prevention specialist workforce can’t drive this population-wide work on their own; however, many people do not know that they are a prevention contributor. As discussed in previous sections, work needs to occur to ensure a shared whole-of-government commitment to preventing family violence, and to generate leadership within non-government sectors. This work will need to build individuals’ understanding that they are prevention contributors. A primary prevention–accredited qualification is being developed for prevention contributors to access through the TAFE sector. This is expected to be a useful addition to the suite of professional learning options for prevention contributors, noting that people will choose a professional learning pathway that best suits their particular context, and the TAFE pathway will not be practical for everyone. It is therefore important to continue to support a range of options for building the primary prevention capability of prevention contributors, including non-accredited training and resources provided by organisations such as Safe and Equal and Women’s Health Victoria.
At the same time, structural levers for increasing uptake of training by prevention contributors need to be considered, such as workplace and industry endorsement of this training as recognised professional development.
Updated