
- Date:
- 12 Dec 2022
This is the sixth of seven topic-based reports, as outlined in the Family Violence Reform Implementation Monitor's plan for 2021–2022.
This report examines the implementation progress in establishing a service system that meets the needs of victim survivors at their point(s) of crisis and supports their journey towards recovery.
Monitoring Victoria's Family Violence Reforms: Crisis response to recovery model for victim survivors
Child and youth friendly report summary
Find our child and youth friendly report summary of the crisis response to recovery for victim survivors. The summary was prepared in partnership with Berry Street’s Y-Change initiative.
Monitoring context
About the Family Violence Reform Implementation Monitor
The Family Violence Reform Implementation Monitor (the Monitor) was formally established in 2017 as an independent statutory officer after the Royal Commission into Family Violence released its report in 2016. The role is responsible for monitoring and reviewing how the government and its agencies deliver the family violence reforms as outlined in its 10-year implementation plan Ending Family Violence: Victoria’s Plan for Change.
On 1 August 2019 former Victorian Corrections Commissioner Jan Shuard PSM was appointed as the Monitor under section 7 of the Family Violence Reform Implementation Monitor Act 2016. Jan took up her role on 2 October 2019, replacing Tim Cartwright APM, the inaugural Monitor.
Monitoring approach
The Monitor’s 2021–2022 plan was developed through a process of consultation with government and sector stakeholders. Topics were selected that aligned areas of greatest interest and concern to sector stakeholders, with reform implementation activity outlined in the government’s second Family Violence Reform Rolling Action Plan 2020–2023. In determining topics, the focus was on areas where an independent perspective could add the most value to the ongoing reform effort.
Topics selected for monitoring throughout 2021 and 2022 are:
- accurate identification of the predominant aggressor
- family violence reform governance
- early identification of family violence within universal services
- primary prevention system architecture
- Aboriginal-led primary prevention and early intervention
- crisis response to recovery model for victim survivors (this report)
- service response for perpetrators and people using violence within the family.
In undertaking our monitoring, the following cross-cutting themes are examined across all topics:
- intersectionality
- children and young people
- Aboriginal self-determination
- priority communities such as LGBTIQ+, people with disabilities, rural and regional, criminalised women, older people and refugee and migrant communities
- data, evaluation, outcomes and research
- service integration.
Monitoring of the selected topics is based on information gathered through:
- consultations with government agency staff
- consultations with community organisations and victim survivor groups
- site visits to service delivery organisations (where possible)
- attendance at key governance and working group meetings
- documentation from implementation agencies, including meeting papers and records of decisions by governance bodies
- submissions made to the Monitor in 2020 by individuals and organisations (many of these are available in full on the Monitor’s website).
Engaging victim survivors in our monitoring
We are also actively seeking to include user experience and the voices of victim survivors in our monitoring. The office is working with established groups including the Victim Survivors’ Advisory Council, Berry Street’s Y-Change lived experience consultants and the WEAVERs victim survivor group convened by the University of Melbourne.
Stakeholder consultation
The Family Violence Reform Implementation Monitor would like to thank the following stakeholders for their time in monitoring this topic:
- Anglicare Victoria
- Boorndawan Willam Aboriginal Healing Service
- Centre for Excellence in Child and Family Welfare
- Commission for Children and Young People
- Court Services Victoria
- Department of Families, Fairness and Housing (includes Family Safety Victoria)
- Department of Health
- Department of Justice and Community Safety
- Dhelk Dja Action Groups – Inner and Outer Gippsland
- Djirra
- Drummond Street
- Eastern Metropolitan Regional Family Violence Partnership
- Economic Abuse Reference Group
- Emma House Domestic Violence Services
- Ethnic Council of Shepparton and District
- FamilyCare
- Federation of Community Legal Centres
- Financial Counselling Victoria
- Fitzroy Legal Service
- Gippsland and East Gippsland Aboriginal Co‑Operative
- Gippsland Lakes Complete Health
- Goulburn Valley CASA
- Mallee Family Care Community Legal Centre
- McAuley Community Services for Women
- NEXUS Primary Health (Broadford)
- Noor Family Violence Survivor Advocates (InTouch)
- No To Violence
- Primary Care Connect (Shepparton)
- Quantum Support Services (Pat’s Place)
- Relationships Australia, Victoria
- Rumbalara Cooperative
- Safe Steps
- Safe and Equal
- Safe and Equal Expert Advisory Panel (survivor advocates)
- The Salvation Army
- Sexual Assault Services Victoria
- Shepparton Specialist Family Violence Court
- Statewide Family Violence Integration Advisory Committee
- Switchboard – Rainbow Door
- The Orange Door – Bayside Peninsula
- The Orange Door – Inner Gippsland
- The Orange Door – Goulburn
- Thorne Harbour Health
- Victim Survivors’ Advisory Council
- Victoria Legal Aid
- Victorian Alcohol and Drug Association
- Victorian Aboriginal Child Care Agency
- Victoria Police
- VincentCare (Shepparton)
- WEAVERs lived experience group (University of Melbourne)
- Western Integrated Family Violence Committee
- Women’s Legal Service Victoria
- Women with Disabilities Victoria.
Foreword

Jan Shuard PSM
Family Violence Reform Implementation Monitor
This topic was all about the victim survivor journey. We wanted to see how well the system was working as a whole to respond to victim survivors at the point of crisis, and its capacity to meet their wide-ranging needs and support them towards recovery. There is no doubt that critical elements of the service system are in place, although there are many areas with insufficient capacity, the most pressing area of need being crisis accommodation. Creating a prompt and seamless pathway for victim survivors navigating their way through these services is also still a work in progress. Understanding demand and providing adequate levels of support to meet presenting needs is central to an effective service pathway for victim survivors. It must be noted that the impact of the pandemic has been a critical factor affecting service delivery, and this report must be considered in this context.
Special thanks to the victim survivors we met with to inform this topic. They so generously shared their experiences to highlight things that worked well for them and areas where improvement was needed. Of note were examples where their experiences were vastly different from pre- to post-reforms, with a much more positive outcome in recent times. It is heartbreaking to hear their stories – the lengths to which they have gone to protect their children and the ongoing trauma they endure. Notwithstanding this, these women are now making an invaluable contribution to the design and delivery of the service response. These champions and advocates are to be admired for their strength and dedication, and their expertise must continue to be harnessed.
I was deeply impressed by the passion and commitment demonstrated by those providing the range of services that support victim survivors on their journey towards recovery. They do amazing work and often go above and beyond to meet victims’ needs as best they can in a tough environment.
But these providers were often under significant demand pressure. There is so much need for services that they cannot keep up, leading to long waitlists and some agencies having to tighten their access criteria. This highlights what we already know about the importance of primary prevention activity to drive down the rates of family violence and reduce demand pressure on these services.
It is critical that victim survivors are appropriately supported to recover from the impacts of family violence, but this is only one part of the picture. The other part is the response to perpetrators, equally critical because without addressing the cause of the violence, victim survivors will struggle to remain safe and recover. It is no mistake that my final two monitoring reports focus respectively on the systems in place to support victim survivors and then the services available to generate behaviour change among perpetrators.
It is always confronting to hear how long many victim survivors have suffered at the hands of people who perpetrate violence against their families before they are able to reach out for help. As described to us, this is always at ‘crisis point’, and the service system has understandably focused its attention on this element to manage risk and keep them safe. However, more needs to be available over the long term to support victim survivors – including children – to heal, recover and thrive.
The family violence service system and related systems continue to support victim survivors every day, and there is excellent practice occurring. There are also areas for improvement, and I hope this report helps to highlight those and instigate systemic changes that support more victim survivors to get their lives back on track and prevent future instances of violence.
A reform agenda of this size and scope is a massive task, and it is a credit to the Victorian Government that it has committed to drive the changes needed. The dedicated public servants, the police, the courts and the family violence sector all work tirelessly to design and deliver the best system they can and respond to emerging needs, and are to be commended for their efforts. To those in the sector delivering services to victim survivors who have informed, embraced and delivered – your devotion to service is outstanding. Finally, to all the victim survivors, including children and young people, who have given their expertise to shape the reforms, your contribution has been awe-inspiring.
Jan Shuard PSM
Family Violence Reform Implementation Monitor
Key findings and suggested actions
Based on our consultations and analysis of key documents, there appears to be an understanding that an ideal response in family violence situations would be swift and holistic, addressing the needs of both victim survivors and perpetrators at the point of their first contact with the system to prevent further abuse. Services would be available at sufficient levels to meet demand and would remain in place for as long as needed for each client while gradually supporting the victim survivor to regain control of their lives.
There are many committed workers, dedicated services and a diligent public service working to improve and support the family violence service system to the extent that they can.
However, the family violence service system faces significant demand pressure, which has been compounded by impacts of the COVID-19 pandemic and ongoing workforce challenges, as are the systems directly related to it (such as the housing, mental health and child protection systems). With reports of family violence incidents remaining high, and so much demand for services, difficult decisions around prioritisation of access and duration of support have to be made.
We found that all parts of the system are experiencing backlogs, and victim survivors are facing less-than-ideal waits to access many of the services they need. We also found that with so much demand, the system is less able to support victim survivors who are not at the highest level of risk, and opportunities to intervene early are sometimes limited. This is problematic because, as victim survivors told us, it takes enormous courage to reach out for support, and it takes even more courage to reach out multiple times after not receiving sufficient support previously.
In addition to these access issues, and while many of the system elements are in place, they have not yet been joined up well enough to provide a smooth journey for the victim survivor. Programs and services are often designed in isolation, with siloed funding and program requirements that make coordination difficult. And while there is guidance for different parts of the system, there is scope to more clearly articulate a ‘crisis to recovery’ model.
While further work is required to improve the system response to victim survivors and support their journey towards recovery, it is exceptionally difficult to ensure victim survivor safety and wellbeing without a strong response to perpetrators. It is vitally important to have effective responses in place to hold perpetrators to account and change their behaviour. This is explored in our companion report covering the service response for perpetrators and people using violence within the family.
We cannot discuss our findings around the family violence response system without very clearly highlighting the utmost importance of strengthening primary prevention efforts. Primary prevention can stop more Victorians from ever having to experience family violence and reduce the demand pressure currently being experienced by the family violence system, thereby allowing it to be better able to meet the needs of the victim survivors presenting to it. Therefore, we must point to the suggested actions included in our Primary Prevention System Architecture report and Aboriginal-led Prevention and Early Intervention report, and the findings and recommendations contained in Respect Victoria’s September 2022 report to parliament: Progress on Preventing Family Violence and Violence Against Women in Victoria.
We also note that, given the integrated approach to family violence prevention, early intervention and response within Aboriginal communities, many of the issues and findings in the Aboriginal-led Prevention and Early Intervention report are also directly relevant to this topic.
Based on our analysis, we make the following high-level findings about the extent to which victim survivors are supported to move from crisis to recovery. These findings form the main sections in this report:
- There is increased visibility of where to go for family violence support, but this is not always leading to improved system access
- Demand pressure on family violence services means many victim survivors can’t access the right supports at the right time
- Workforce challenges are substantially affecting service delivery
- Navigating the family violence and related systems remains a challenge for victim survivors, but there are some good examples of coordination
- Victim survivors are accessing a range of systems and services that often struggle to keep pace with demand
- Longer term support and a more holistic approach are required to support recovery and healing.
To address these matters, we suggest a series of actions (see Figure 1) that will need to occur alongside ongoing efforts to build capacity across workforces, improve intersectional responses, monitor and evaluate progress, and embed the Family Violence Multi-Agency Risk Assessment and Management (MARAM) Framework and information sharing reforms.
Figure 1: Proposed actions to improve the response to victim survivors, from crisis to recovery
Victim-centred approach to service delivery and design
- Implement a clear model for cross-sector referrals, secondary consultations and service coordination to improve system integration, defining the service responsible for supporting a victim survivor to navigate systems.
- Identify more opportunities for service co-location or collaboration, particularly between police, courts and The Orange Door or other specialist family violence services. This should include consideration of a co-responder model for Victoria Police.
- Take specific actions to enhance the regard for children and young people as victims in their own right, including safely giving them a greater voice during family violence–related court proceedings.
- Continue to advocate for reform by the Australian Government in areas such as immigration law, Medicare, Centrelink and the family law system to remove the known barriers in these systems to victim survivor support and recovery.
Access to the supports victim survivors need
- Actively work to embed financial counselling and legal assistance into the family violence response model.
- Facilitate the broader use of peer support as part of the recovery process for victim survivors.
- Articulate the role of the mental health system in supporting victim survivor recovery and drive stronger coordination between the mental health and family violence systems.
- Review the male victim survivor pathway, and consider where a dedicated male victim survivor response should be located and how it can link with more specialised supports.
Workforce
- Drive improved conditions for family violence and sexual assault sector workers, including by targeting the structural causes of insecure work and low pay.
- Consider additional support that organisations may require to fully understand and apply the equivalency principles of the Mandatory Qualifications Policy.
- Leverage insights from the mental health lived experience workforce to inform a framework and career pathways for the family violence lived experience workforce.
Funding
- Explore opportunities to adopt client-centred funding models that improve service continuity and coordination.
- Continue to advocate for increased investment in the range of services victim survivors need, such as:
- housing from crisis accommodation to long-term affordable accommodation, and other options for supporting victim survivors to maintain rent and mortgages
- therapeutic interventions
- legal and financial advice and advocacy.
Data and monitoring
- Strengthen the availability of data across the system, including wait time, support provided and outcomes across The Orange Door, case management services and therapeutic services.
- Regularly analyse victim survivor journeys through the system to identify issues or blockages, particularly for groups such as children and young people.
- Establish a formal monitoring framework across The Orange Door sites to ensure quality and consistency with the service model, and identify possible sources of service delays.
Introduction
Ensuring there is an appropriate system in place to meet family violence victim survivors’ immediate and longer term needs is vital in allowing them to get their lives back on track and prevent further abuse. In investigating this topic, we sought to examine the implementation progress in establishing an effective service system that meets the needs of victim survivors at their point(s) of crisis and supports their journey towards recovery. Specifically, we explored:
- how victim survivors experience the service system from the point of crisis and beyond
- the extent to which the range of services a victim survivor might need are available, accessible and wellcoordinated
- the extent to which the service system meets the needs of diverse groups
- whether there is enough focus on long-term recovery.
We note that the family violence service system considers a victim survivor as being in crisis when they require immediate support to respond to a threat posed by a perpetrator. This report includes discussion of the support available at such a point of acute family violence crisis. However, we are also guided by the victim survivors we met who explained that ‘if you’re ready to get help and you reach out, you are in crisis and need that help’. This report also, therefore, explores what happens when a victim survivor reaches out to the family violence service system for help, or when police become involved, whether or not the system considers them to be in crisis.
When we say ‘recovery’, we are talking victim survivors being able to heal so that their past trauma doesn’t continue to have an overwhelming impact on their lives, as evidenced by improvements to their health, safety, wellbeing and participation in society. We fully acknowledge what some victim survivors have told us: that you don’t ever fully recover from the experience of family violence. In that context, we focus throughout this report on how victim survivors are supported on their journey towards recovery. We also acknowledge that this journey is not always linear. For example, a victim survivor’s situation may stabilise, but they may re-enter the crisis phase if they return to a relationship with a partner who uses violence. This may, at times, be linked with delays or barriers to them being able to access the services they need to maintain stability and move towards recovery.
Scope
We acknowledge that victim survivors will disclose family violence and connect with the family violence system in a range of ways; however, it is not possible nor practical for us to explore all these pathways in this report. Some of these pathways are captured in our Early Identification of Family Violence Within Universal Services report, which explored how well mainstream health and education services are able to identify family violence and connect victim survivors with the support they need. The scope of this report is limited to situations where police have become involved or a victim survivor has reached out to the family violence system for support.
Context
As always, we must highlight the challenges that ever-increasing levels of demand and the added pressure of COVID-19 have had on the family violence sector. The sector representatives we met with are exceptionally committed to supporting victim survivors and to improving the system, and they often go over and above to meet the needs of their clients. The findings and suggestions in our report must be taken in this context.
What did the Royal Commission say and what has changed since?
The Royal Commission made several overarching findings that relate to effective system responses to victim survivors. Among a series of system limitations, it made the following findings that directly affect the victim survivor journey towards recovery (see Figure 2).
Figure 2: System limitations identified by the Royal Commission most relevant to the victim survivor journey
- All parts of the system (support services, police, courts) are overwhelmed by the number of family violence incidents now reported. Services are not currently equipped to meet this high level of demand, which undermines the safety of those experiencing family violence and their potential for recovery.
- The range of services a victim might need at different times, including at points of crisis and beyond, are not as well coordinated as they should be, particularly when these services are located in different systems—for example, the health and justice systems. Gaining access to support can be difficult for victims, and service responses remain inconsistent and hard to navigate.
- The current response to family violence largely assumes that women will leave their home when family violence occurs. For those who must leave, homelessness and housing systems cannot guarantee a safe place to stay or a permanent home that is affordable. For those who remain at home, monitoring of the perpetrator is inadequate.
- The many different forms and manifestations of family violence are insufficiently recognised, and responses are not tailored to the particular circumstances and needs of diverse victims.
- There is a lack of targeted resources to meet the specific needs of children and young people who have experienced family violence.
- …there is not enough focus on helping victims recover from the effects of violence and rebuild their lives.
Source: State of Victoria (2016): Royal Commission into Family Violence: Summary and Recommendations, Parl Paper No. 132, p. 6.
The Royal Commission also made several recommendations that relate to support for victim survivors of family violence from the point of crisis and beyond. These recommendations reflected the need to:
- improve safe and stable housing options, including supporting victims to safely remain in, or return to, their homes and communities, and ensure there are appropriate options to meet the needs of children and young people
- improve service pathways by introducing a network of support and safety hubs
- provide more funding for specialist family violence services and Aboriginal Community Controlled Organisations to meet demand
- provide more funding for therapeutic interventions and counselling for children and young people
- expand the provision of Family Violence Flexible Support Packages
- partner with Aboriginal communities to develop a strategic response to improve the lives of Aboriginal children and young people and provide support to Aboriginal parents
- ensure greater collaboration between family violence services and others including mental health, alcohol and other drug, and child protection services
- address the needs of diverse groups
- strengthen investment in recovery by:
- supporting victim survivors’ health and wellbeing (including by ensuring access to counselling)
- supporting victim survivors’ financial security (including by expanding the delivery of financial literacy training for victim survivors).
Since then, substantial effort has gone into improving a range of systems to better respond to the needs of victim survivors. The Victorian Government has invested in therapeutic interventions for victim survivors, safe housing including improved crisis accommodation, and training for a range of workforces. A range of strategies and commitments have been made, all of which aim to improve the experiences of and outcomes for victim survivors. For example:
- Ending Family Violence: Victoria’s 10-year Plan for Change (2016) outlines the government’s response to the Royal Commission and its overarching approach to family violence reform in Victoria. Most relevantly, it commits to:
- designing the system and services to keep children safe
- taking a whole-of-family approach to stopping violence, keeping victim survivors safe from harm, and helping them to recover from the experience of violence
- providing safe and stable housing
- supporting longer term recovery with employment, financial security, legal assistance, educational opportunities and supports for emotional and mental health needs.
- The 10-year plan also introduced the Family Violence Outcomes Framework, which was intended to be a tangible tool to ensure accountability for achieving intended outcomes, and to which all parts of the reform were to be linked. Two of the domains directly address the response to victim survivors and include indicators relating to victim survivor safety, agency and recovery, as well as a more integrated and person-centred system, backed by a skilled workforce (see Figure 3).
Figure 3: Relevant domains and indicators from the Family Violence Outcomes Framework
| Domain 2: Victim survivors, vulnerable children and families, are safe and supported to recover and thrive | Domain 4: Preventing and responding to family violence is systemic and enduring |
|---|---|
| Early intervention prevents escalation — people, including children and young people, at risk of witnessing or experiencing family violence are identified early and provided with effective early interventions. | The family violence system is accessible, and services and programs are available and equitable — Prevention activities occur across all key settings and the support system is easy to navigate and services are available to people when and where they need them, at all times of the day and night. |
| Families are safe and strong — the system intervenes early to prevent harm to children and young people and enables families to access effective support services when they need them. | The family violence system intervenes early to identify and respond to family violence — The family violence system intervenes and responds early to prevent escalation and minimise harm and risk for people using family violence and those at risk of using family violence. |
| Victim survivors are safe — the system takes responsibility for managing risk, instead of placing the onus on victim survivors, including children and young people. | The family violence system is person-centred and responsive — services are personalised, flexible, culturally relevant and reflect individual and family choices, need and circumstances, particularly for diverse communities and those with complex needs. |
| Victim survivors are heard and in control — victim survivors, including children and young people, are always listened to, believed and understood, and supported to take control of their immediate situation and make decisions about their future. | The family violence system is integrated — services work together and share information to provide a coordinated quality response to people and families, informed by dynamic risk assessment and sensitive to people’s diverse needs. The system supports effective and evidence-based prevention efforts. |
| Victim survivors rebuild lives and thrive — disruption is minimised for victim survivors, including children and young people, with safe and secure housing, finances, employment, education and recovery from trauma available for as long as people need it. | The family violence and broader workforces across the system are skilled, capable and reflect the communities they serve — the workforce is supported through new career pathways, fair conditions and a commitment to enhanced wellbeing and safety, and is skilled to meet people’s diverse needs. |
Source: Family Violence Outcomes Framework.
- The Family Violence Rolling Action Plan 2017–2020 began to put the 10-year plan into action. It committed to a range of actions including creating Family Safety Victoria, the rollout of support and safety hubs (now known as The Orange Door network) and a range of workforce capacity-building initiatives. It also flagged development of a new demand modelling tool ‘to provide a robust picture of current and future demand for family violence and related social and justice services’ that victim survivors need, and a new funding approach that allows for more flexible and tailored service delivery.
- The Family Violence Reform Rolling Action Plan 2020–2023 seeks to further embed the reforms and organises its actions according to a selection of priority areas that impact on the experience of victim survivors, including housing, The Orange Door network, legal assistance and workforce development.
- The Dhelk Dja: Safe Our Way – Strong Culture, Strong Peoples, Strong Families Agreement 2018 includes priority 3: ‘self-determining Aboriginal family violence support and services’. Under this priority, the agreement explains that services ‘need to intervene early to prevent harm and wrap-around a person, child or family to provide a response from crisis to healing, addressing all of their safety and wellbeing needs, including housing and legal needs’. This complements broader frameworks and agreements designed to drive self-determination and improve outcomes for Aboriginal people, including the Victorian Aboriginal Affairs Framework 2018–2023 and the National Agreement on Closing the Gap.
- Everybody Matters: Inclusion and Equity Statement, released in 2019, complements Ending Family Violence and outlines the government’s commitment to building an ‘inclusive, safe, responsive and accountable family violence system for all Victorians’. A key part of this is adopting an intersectional approach at all levels of service delivery, thereby acknowledging and responding to the intersecting range of needs a victim survivor might have, based on factors such as their Aboriginality, gender, sexual orientation, ethnicity, religion, disability and mental health.
- Specific headline reforms include:
- the MARAM Framework, which continues to be implemented to improve consistency in the way family violence is understood and responded to across the family violence and related sectors
- the Family Violence Information Sharing Scheme, which is increasingly being used to share information about victim survivors and perpetrators between information sharing entities to improve service responses to victim survivors and maximise their safety and wellbeing
- The Orange Door network, which has been established in all 17 Department of Families, Fairness and Housing regions in Victoria, acting as the primary entry point to the family violence system and related supports and providing a clear point of contact for victim survivors
- Specialist Family Violence Courts, which are designed to provide a more specialised, trauma-informed approach to court design and operations, and are now operating in 12 locations across the state
- the creation of local Family Violence Investigation Units and the Victoria Police Family Violence Centre of Learning, among other targeted initiatives, to improve the way police respond to family violence incidents and better meet the needs of victim survivors.
Initiating support
There is increased visibility of where to go for family violence support, but this is not always leading to improved system access
There are very clear entry points into the family violence service system for most victim survivors seeking help: Victoria Police, The Orange Door and the Safe Steps Family Violence Response Centre. It is a great achievement that awareness of what family violence is and where to go for assistance appears to be increasing. However, likely because of that awareness, demand pressure continues to increase (see Figure 4 and Figure 5), and we heard numerous accounts of victim survivors experiencing long waits to have their risk and needs comprehensively assessed at The Orange Door, except in the most serious cases. Furthermore, some groups of victim survivors face additional barriers to linking in with the family violence service system.
There are some clear areas for improvement, including the need to streamline intake and assessment processes at The Orange Door, reconsider the service pathway for male victim survivors, and more effectively communicate with groups that may be more likely to self-exclude from The Orange Door and the family violence system more broadly.
Figure 4: Family violence incidents recorded by Victoria Police

{kind=link}
Police response and referrals
Victoria Police has comprehensive guidance in place for members responding to family violence incidents. This guidance is captured in the Victoria Police Manual: Family Violence, Code of Practice for the Investigation of Family Violence, and a range of practice guides. Victoria Police’s Family Violence Options Model, contained in the code of practice, clearly articulates that the actions taken should aim to support: safety for adult and child victims, appropriate referrals being made, the prevention of future family violence, and investigation and prosecution of perpetrators where appropriate.
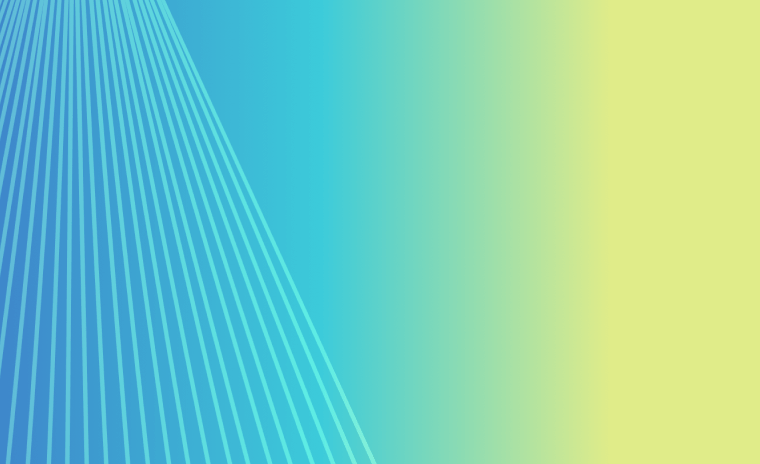
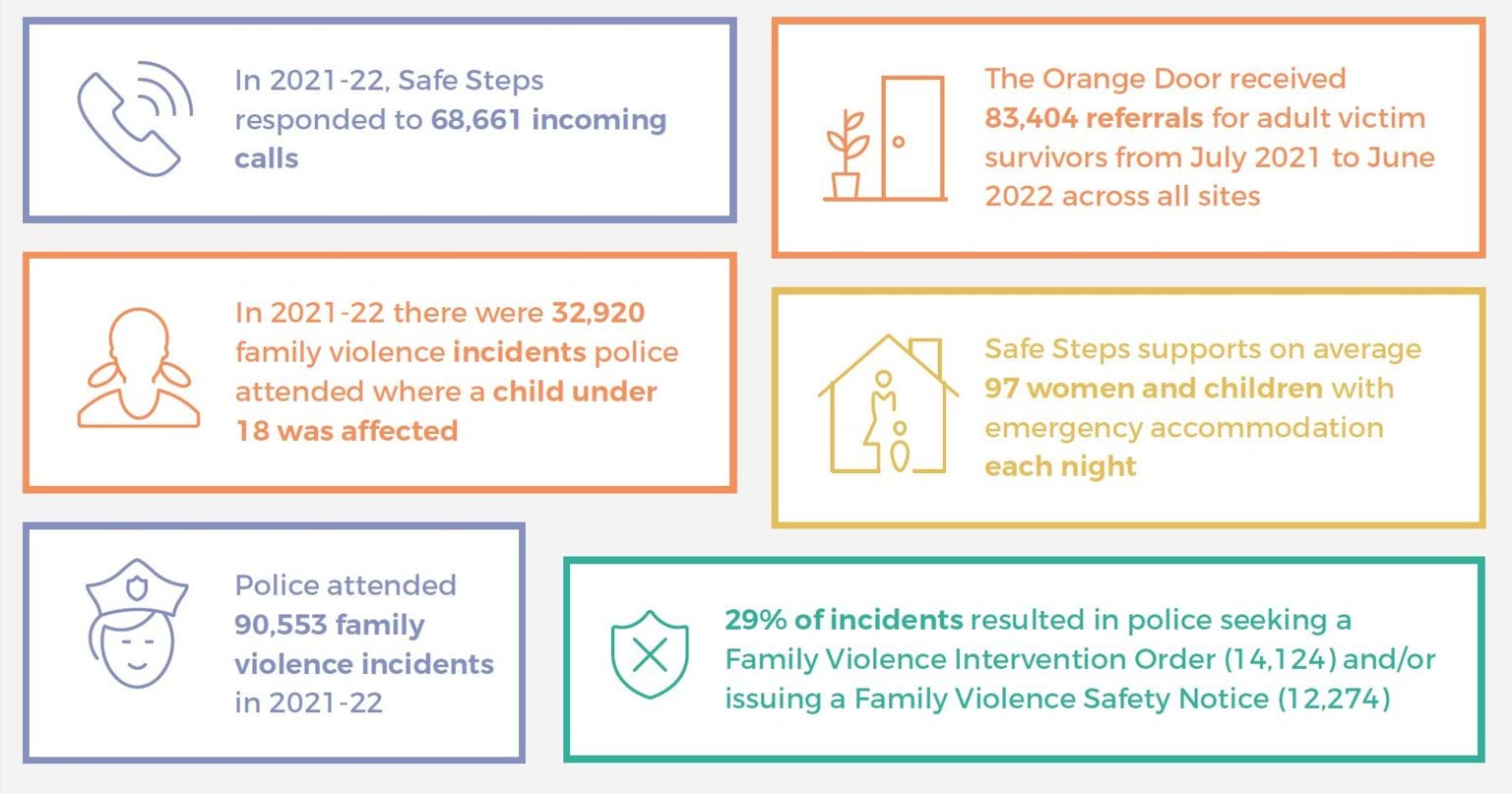
Figure 5: Highlighted statistics demonstrating the need for family violence support
{kind=link}
Child safety is a priority in the guidance, with the Victoria Police Manual being clear that members are expected to assess the interests of the child independently of a parent. Police members are also expected to respond effectively to the diverse needs of priority populations, with the Family Violence Priority Community and Diverse Community Responses practice guide outlining, among other things, barriers to reporting and recommended police practice for engaging with a number of priority groups in the community. The code of practice is clear that ‘Victoria Police recognises the importance of an intersectional approach when responding to and investigating family violence across our diverse Victorian community’.
Family violence and Child Protection referrals are also clearly described in police materials:
- Referrals to family violence services are automated through the Family Violence Report (L17) portal, where there are immediate concerns for the safety and welfare of victim survivors. Alternatively, where there are no immediate concerns, victim survivors are provided with information on who they can call, as part of an ‘informal referral’. Formal referrals appear to be far more commonly used, however, with 81,048 formal referrals for affected family members across all police regions in 2020–21, in contrast with 10,785 informal referrals.1
- Mandatory reports to Child Protection are required ‘as soon as practicable after forming a belief on reasonable grounds that a child has suffered or is likely to suffer significant harm as a result of physical injury or sexual abuse, and the child’s parents are unable or unwilling to protect the child’.2 Members are also asked to consider reporting to Child Protection where children have suffered or are likely to suffer significant harm as a result of other forms of abuse or neglect. In 2020–21 police attended 33,948 family violence incidents involving children (7,834 incidents where a child was recorded as the affected family member and 27,639 incidents where a child was recorded as witnessing family violence).3 In the same year, police made 4,098 direct referrals to Child Protection and 6,942 direct referrals to Child FIRST.4 In addition, where a formal referral via the L17 portal is made but the threshold for a direct referral to Child FIRST or Child Protection is not met, the specialist family violence services and the Victims of Crime Helpline receiving the formal referral will consider the need for children involved to be referred, and will make referrals if appropriate. There are multiple opportunities for referral to Child Protection and Child FIRST, and children may also receive support through family violence, therapeutic and other services, but as discussed throughout this report, gaining access to these services can be difficult, and we are concerned that many children experiencing family violence may not be receiving direct support at all.
- Victoria Police has a separate e-referrals system for referrals to other services including legal, youth and mental health services. It is not clear how often such referrals are made.
While Victoria Police guidance is comprehensive, practice that matches the strategic intent does not always occur, as discussed in detail in our Accurate Identification of the Predominant Aggressor report. Stakeholders including Victoria Police and the Coroners Court of Victoria explained that public expectations of police responses to family violence are increasing, while the number of family violence incidents is also on the rise. To address this challenge, one model that has been suggested and trialled in some locations is a co-responder model, whereby a social worker attends family violence incidents together with police. Once such model is the Alexis – Family Violence Response Model, which was co-designed by Victoria Police and The Salvation Army, in collaboration with other local stakeholders. It involves an Alexis Senior Family Violence Practitioner from The Salvation Army being physically located within the local Victoria Police Family Violence Investigation Unit, and provides a coordinated, multi-agency response to families who are having repeated contact with police and services due to family violence. The initiative has been evaluated and shows promising results, including a reduction in family violence incidents for families receiving the Alexis response, and vastly improved victim survivor engagement with social services (see Box 1 for an example). As the Coroners Court of Victoria told us:
Given the ongoing challenges faced by the sector in providing victims of family violence with an appropriate response, the State Coroner is currently exploring whether the expectations placed on police when responding to family violence are realistic and how victims may be better supported to engage in family violence services. As a part of this consideration, the State Coroner is working with the [Victorian Systemic Review of Family Violence Deaths] Review Panel to explore the benefits and utility of a state-wide co-responder model.
We would support such exploration and suggest it may be a way to ensure improved engagement of victim survivors with the family violence service system, who may not otherwise engage following police attendance at an incident, despite any referrals made [relates to action 2].
Box 1: The Alexis-Family Violence Response Model in action
Roxy was a 47-year-old inpatient at a public hospital being treated for breast cancer in 2021. The hospital Roxy was attending systemically responds to family violence - including actively using MARAM and information sharing provisions - with the support of the Strengthening Hospital Responses to Family Violence initiative. Hospital staff referred Roxy to the local Victoria Police Family Violence Investigation Unit (FVIU) because she was facing a range of challenges, including physical and mental ill-health (with a history of suicide attempts), unstable and transient housing, and disclosures of family violence. Roxy was still in a relationship with the perpetrator and was experiencing ongoing physical, psychological and financial abuse and controlling behaviours. The FVIU that received the referral included co-located specialist family violence practitioners from The Salvation Army under the Alexis Family Violence Response Model.
The intervention commenced with police and Alexis workers attending the hospital jointly to meet with Roxy, who detailed her background, relationship history, current concerns and stressors. Roxy was not initially seeking formal intervention by police but was receptive to ongoing informal police support and assistance from Alexis workers with her self-identified ultimate goal of separation from the perpetrator.
Throughout the duration of the support period, a care team approach to intervention was taken, bringing together Alexis practitioners, police, housing support, hospital staff and mental health services. Collectively, the care team provided support such as:
- psychoeducational and emotional support around family violence
- risk management planning, conducted at the hospital directly after cancer treatment sessions, to avoid the perpetrator knowing about them
- completion of a Victorian Housing Register application for social housing
- police and legal advocacy around the Family Violence Intervention Order process
- support to re-establish relationships with estranged family members
- support with re-entering education.
Seven months after referral, Roxy was in remission following surgery and cancer treatment. Her mental health was reported to be currently stable. She had separated from the perpetrator and a three-year Family Violence Intervention Order had been put in place. Roxy was in women’s supported accommodation and she was expected to shortly receive ongoing housing. Roxy has since reconnected with family members and re-entered education to pursue a career in mental health peer support.
Source: Based on a case study provided by The Salvation Army.
Crisis response model
Building on the previous after-hours response model, Family Safety Victoria has developed a crisis response model in consultation with the sector. The model is now finalised, approved and being distributed across the sector, and alignment is expected by 1 April 2023. The model is captured in three documents:
- the Case Management Program Requirements (discussed in the next section)
- Roles and Responsibilities After Hours
- Role and Responsibilities in Providing Emergency Accommodation.
According to the Case Management Program Requirements, a crisis response is an ‘urgent, rapid intervention to mitigate risk and harm for victim survivors’. This response is for victim survivors identified to be at serious risk of harm and with urgent safety needs. A crisis response can be initiated by Safe Steps, The Orange Door or a local specialist family violence service, although Safe Steps offers an all-hours service. Child Protection also delivers an all-hours service to respond to children and young people at risk, including those facing an immediate risk of harm due to family violence.
Safe Steps responds to any victim survivor who calls seeking help through its all-hours phone line or live chat support, providing, at a minimum, risk assessment and safety planning. Safe Steps responded to 68,661 calls in 2021–22, with an average time on hold of approximately two minutes. This suggests that despite significant demand, victim survivors who are calling for help are getting to speak to a specialist family violence practitioner promptly.
As might be expected, stakeholders told us that victim survivors with the most urgent needs are receiving the timeliest and most effective responses from the service system. Where victim survivors face an imminent threat, various parts of the system (including, for example, Victoria Police, Safe Steps, The Orange Door and crisis accommodation services) work together to swiftly get the victim survivor(s) to safety.
Despite the positive feedback, there are some very real challenges for staff providing crisis responses to victim survivors in immediate danger. One challenge is the incompatibility of information systems being used by different parts of the system. For example, The Orange Door and Safe Steps use different client management systems, so when a crisis response transfers from The Orange Door during business hours to Safe Steps for an after-hours response, information has to be manually handed over, or risk assessments have to be repeated.
Another challenge is finding appropriate emergency accommodation. A refuge eligibility and prioritisation framework has been developed to clarify how applications for refuge should be prioritised and confirm a central coordinating role for Safe Steps. This will likely be helpful in making prioritisation decisions; however, the vast majority of victim survivors will not be able to access refuge at all. We heard that many victim survivors are in crisis but don’t meet the urgency criteria for refuge accommodation, yet if they seek general homelessness support, they are told they need a crisis response. For young people fleeing violence on their own, we were advised that there are very few options.
Many stakeholders, including victim survivors, said that clients with alcohol and other drug (AOD) issues are told they must be ‘clean’ for six weeks before they can receive crisis accommodation. Through the Victorian Alcohol and Drug Association, we also received numerous examples of clients using alcohol and/or other drugs (some of whom are coerced to do so by their perpetrator) being denied a crisis response service and adequate protection through the family violence system, despite risk being identified by AOD clinicians. We suggest there is room to improve the capability of the family violence system for clients who use AOD to ensure they can access appropriate support.
The excess demand for refuge places has led to a reliance on motel accommodation. For example, Safe Steps has advised that in 2021–22 it accommodated 3,124 unique clients, and despite 72 per cent being classed as ‘serious risk’ or ‘serious risk requiring immediate protection’, 90.8 per cent of cases were accommodated in motels. The use of motels has been widely criticised,5 but in the absence of any other options, it has become a necessity. The new crisis response model appears to begin to respond to past concerns (which were reflected in our 2020 report) about victim survivors accommodated in motels being insufficiently supported. The model aims, in part, to ensure all victim survivors in emergency accommodation have access to face-to-face support from a specialist family violence service and are supported in their transition out of emergency accommodation. However, the Statewide Family Violence Integration Advisory Committee remains concerned about:
…. increasing numbers of women and children residing in inappropriate and unsustainable crisis accommodation … for extended periods of time with only ‘brief intervention’ support whilst awaiting specialist family violence case management allocation.
Although more work is required, substantial efforts are being made to improve the suitability of emergency accommodation options for victim survivors. For example:
- The Refuge Redevelopment Program is replacing 17 communal refuges with ‘core and cluster’ designs and constructing another three Aboriginal-designated refuges. There have been some implementation delays due in part to COVID-19 and rising costs of building materials, but as of 8 November 2022, 13 of the sites had been completed and handed over to agencies. The core-and-cluster design is more suitable for families and women with disabilities. However, as Women with Disabilities Victoria pointed out, for example, the low benches that have been installed in some of the units to support those requiring them are not height adjustable and therefore won’t suit a range of needs. We suggest ongoing engagement between government and the agencies delivering the refuge services to identify areas for improvement and refinement.
- The Motels Coordination Initiative is a year-long initiative that began in June 2022. It is working to identify and address key issues with using motels (or other private accommodation) as emergency accommodation. The initiative acknowledges that while motels are an option of last resort, their use is required to meet excess demand. The initiative is driven by funded Local Family Violence Motel Coordination Projects in each of the 17 Department of Families, Fairness and Housing areas, which aim to identify local area solutions and opportunities for improvement, and a Statewide Reference Group, which is responsible for considering more strategic responses to issues and making recommendations.
- Safe Steps and Safe and Equal have developed advice for services providing crisis responses to guide relationship management with moteliers and to identify preferable emergency accommodation characteristics.
Another important part of the crisis model is brokerage funding. During consultations for this report, as well as for past reports, stakeholders have spoken about the benefits of being able to mobilise brokerage funding for victim survivors to promptly and flexibly access supports to meet their needs. Currently, we are aware of three such sources of brokerage that can be used to support victim survivors to transition out of crisis: flexible support packages, crisis brokerage and the Disability and Family Violence Crisis Response Initiative (DFVCRI). The DFVCRI, which we are advised has ongoing funding, is accessible through Safe Steps’ family violence specialist disability liaison officers and is pivotal in allowing the system to meet the urgent needs of victim survivors with disabilities seeking safety from family violence situations. This is because the National Disability Insurance Scheme cannot provide responses to immediate disability-related crisis needs. Safe Steps and Women with Disabilities Victoria have advised that there is considerable room for improvement in ensuring more people are aware of the initiative so it can be more widely used.
The Orange Door
The Orange Door network is now operating in all 17 Department of Families, Fairness and Housing areas in Victoria, so no matter where a person lives in the state, they can access support through The Orange Door. Looking at data from the past year, referrals and presentations to The Orange Door have remained relatively consistent over time, given the increasing number of sites (see Table 1).
Table 1: Referrals for children and adult victim survivors to all active The Orange Door locations, July 2021 to June 2022
| Month | Jul | Aug | Sep | Oct | Nov | Dec | Jan | Feb | Mar | Apr | May | Jun |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Child referrals* | 5253 | 6389 | 6029 | 6027 | 8570 | 8493 | 7296 | 8700 | 10118 | 8690 | 10240 | 10004 |
| Adult victim survivor referrals | 4578 | 5019 | 5212 | 5555 | 7281 | 7750 | 7222 | 7690 | 8685 | 7457 | 8785 | 8170 |
| Number of sites operating | 8 | 9 | 10 | 11 | 13 | 13 | 13 | 14 | 14 | 14 | 15 | 15 |
*Child referrals include children referred for family violence reasons and/or wellbeing concerns. During this period, approximately 20 per cent of children referred to The Orange Door proceeded to the assessment stage and were found to be victim survivors.
Source: Data provided by Family Safety Victoria.
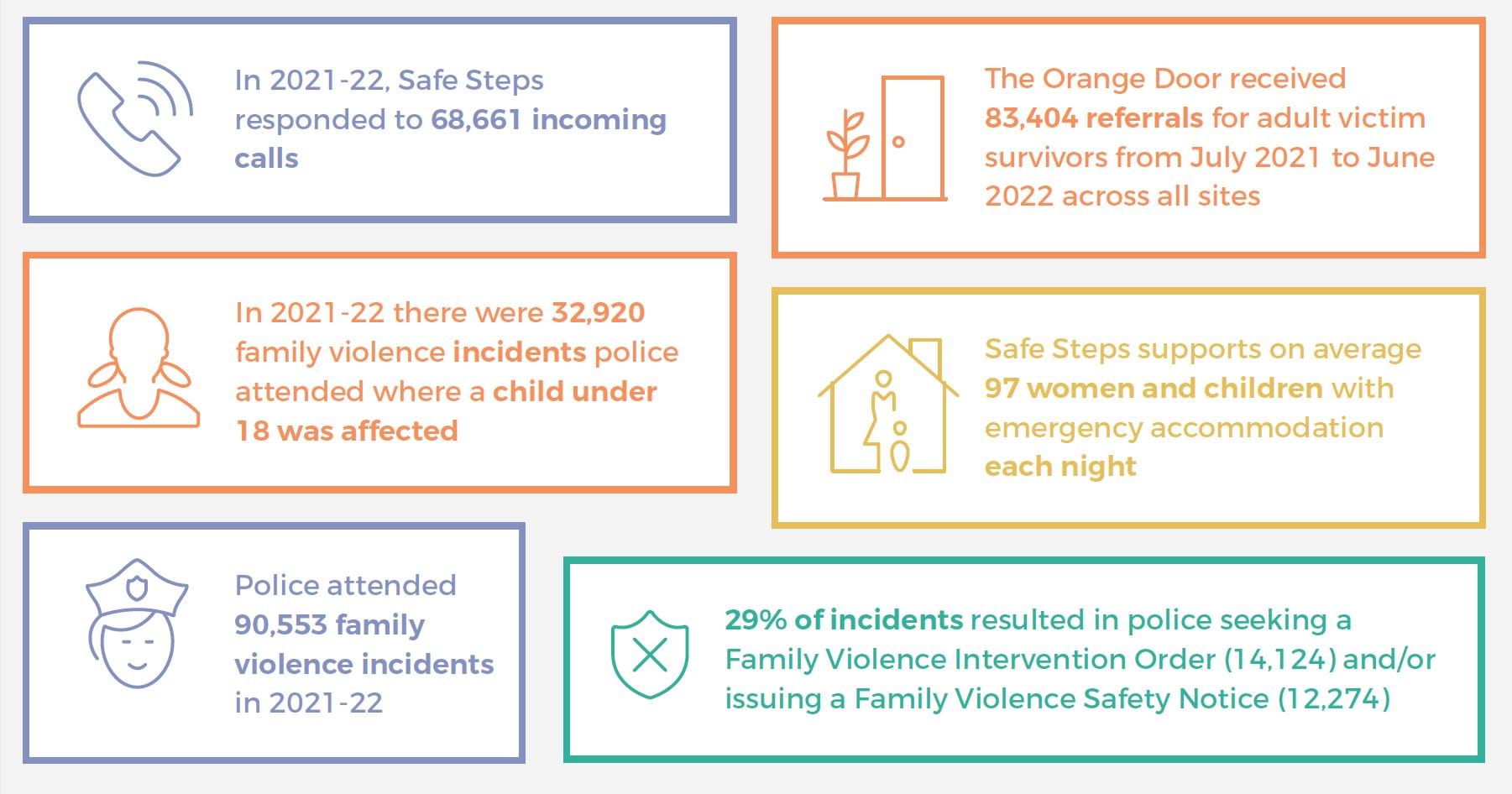
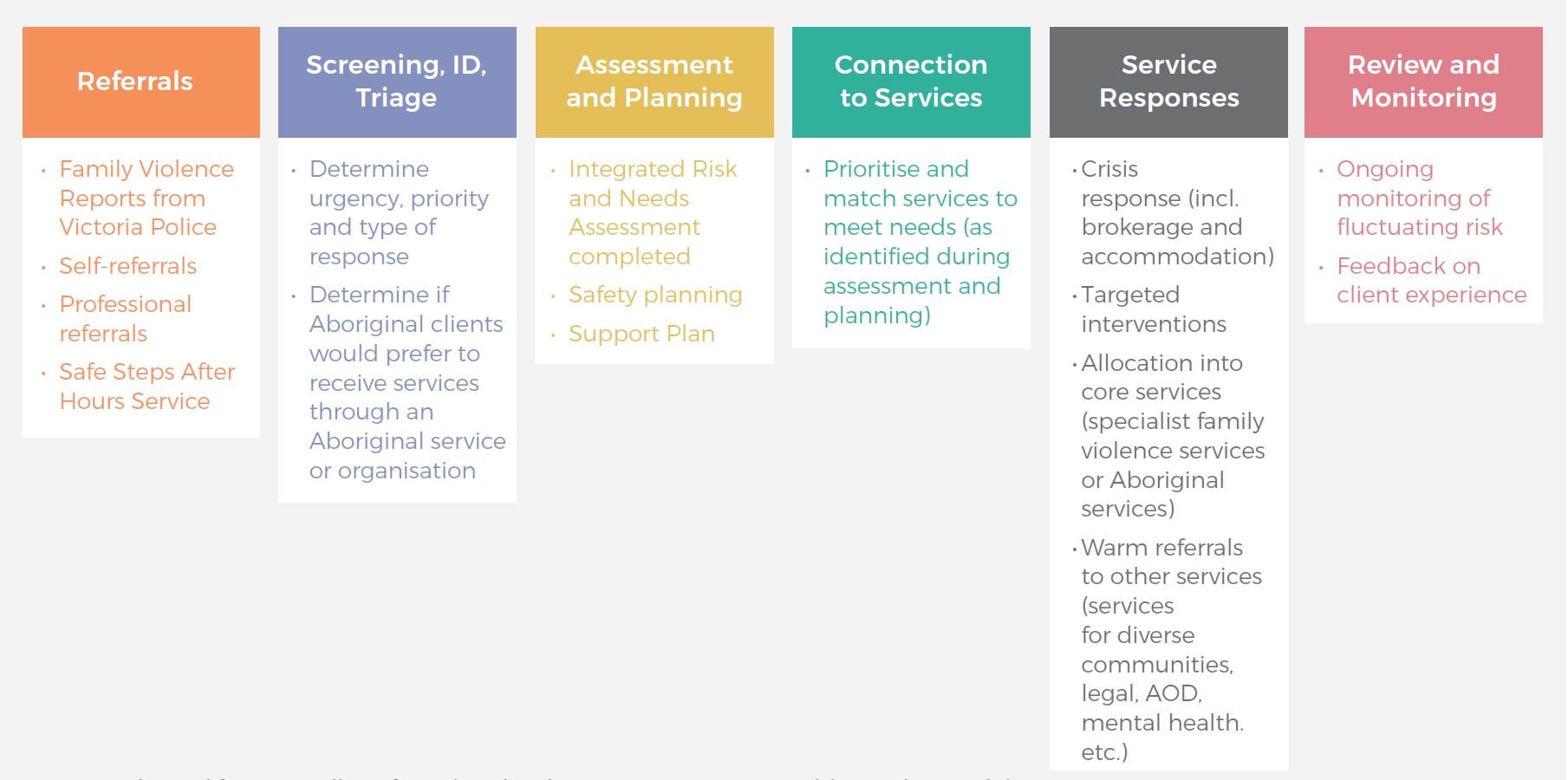
Based on our consultations, there was broad support for The Orange Door model and its potential to ensure a clear and consistent process for intake into the family violence service system. Indeed, we were highly impressed by The Orange Door practitioners we met across multiple sites during this monitoring period. They spoke with a great deal of expertise, understanding of the key challenges and commitment to improving the way victim survivors’ safety and wellbeing could be supported. As it has been described to us, The Orange Door service model is logical, thorough and designed to prioritise victim survivors at greatest risk (see Figure 6). In practice, however, multiple stakeholders have raised issues and areas for improvement. These are explored below.
Figure 6: The Orange Door service model
{kind=link}
Most commonly, stakeholders spoke about processes within The Orange Door taking much longer than expected, leading to bottlenecks in victim survivors being able to access case management support from specialist family violence services. It is difficult to get a very clear picture of the extent of these delays and what is causing them [relates to action 14]. The data we have seen shows that triage (which involves checks of the available databases to look at the pattern and history of violence) occurred, on average, within three and a half days during 2021–22. The average wait time between referral and having a case worker assigned was 11.8 days across April to June 2022 (see Table 2). More detailed investigation would be required to explore wait times for assessment and whether there are particular groups for whom delays are more common [relates to action 16].
Table 2: Triage priority for child and adult victim survivors, and average wait times
| Tier (as determined at assessment stage) | Proportion of victim survivors | Average time from referral to triage finalisation - ADULT | Average time from referral to triage finalisation - CHILD | Average time from referral to assessment - ADULT | Average time from referral to assessment - CHILD |
|---|---|---|---|---|---|
| Tier 1 | 65% | 2.7 days | 3.2 days | 8.4 days | 8.5 days |
| Tier 2 | 27% | 4.4 days | 4.3 days | 18.2 days | 14.8 days |
| Tier 3 | 8% | 3 days | 3.6 days | 10.8 days | 10.8 days |
| All tiers | 100% | 3.4 days | 3.6 days | 11.3 days | 10.3 days |
Note: Tier 1 is the highest priority. Time to triage finalisation based on the average from July 2021 to June 2022. Time from referral to assessment (where client is assigned a worker) is based on the average from April-June 2022.
Source: Data provided by Family Safety Victoria
We were also frequently told that there is considerable variation across The Orange Door sites – that ’every site does it differently’. While some local variation is to be expected, a key aim of The Orange Door is to ensure greater consistency of response wherever a victim survivor accesses the service system.
While we understand that The Orange Door accepts all victim survivors, many victim survivors and third-party professionals we have spoken to this year reflected experiences where victim survivors are referred to The Orange Door but ultimately do not meet the threshold for support, leaving them feeling discouraged. Further investigation is required to determine where this perception of a ‘threshold’ is coming from.
The Orange Door is also explicit about wanting to offer ‘accessible, responsive and non-discriminatory supports tailored to individual needs and experiences’; however, some victim survivors are reluctant to access The Orange Door. For example, we were told that older people experiencing family violence will usually see The Orange Door (and family violence services more broadly) as being for younger women and children and will self-exclude. Many stakeholders raised the presence of Child Protection within The Orange Door as being a deterrent to some victim survivors reaching out to the service. This was particularly relevant for Aboriginal clients and clients with a disability, who had heightened concerns about potentially having their children removed from their care, although we note that these concerns existed even before the introduction of The Orange Door model. It is, therefore, important to continue to build trust and capability within mainstream family violence services (see, for example, Box 2) to better respond to diverse needs, and to support all services, including by having a clear approach to referrals, secondary consultations and coordination [relates to action 1]. For example, several Aboriginal Community Controlled Organisations advised that mainstream services working with Aboriginal clients do not consistently seek secondary consultations or share information with them. The Victorian Aboriginal Child Care Agency has indicated that more work is required to improve the response system to ensure services are culturally safe, and it recommends that minimum standards on cultural safety for the mainstream sector are developed, implemented and reported on.
Equally important is the need to retain the ‘no wrong door’ approach that effectively links victim survivors with support wherever they feel comfortable accessing the system (for example, The Rainbow Door, Seniors Rights Victoria and Aboriginal Access Points). Many Aboriginal Community Controlled Organisations spoke of the need for improved data about family violence and its links with other issues within their communities, to inform stronger planning for self-determined, holistic service delivery.
Box 2: Case example: establishing risk with a victim survivor with a disability
Maggie presented to The Orange Door seeking family violence support. She has a cognitive disability, and in her initial risk assessment, Maggie reported that her partner Stephen was mean to her dog, and that he would take the dog outside and tie him up. This was noted in her original referral report with no further context.
Due to her disability, The Orange Door referred Maggie to a private practice family violence consultant. Maggie had a number of sessions with the consultant, where the consultant built trust and was able to take the time and find ways to communicate appropriately with Maggie.
During the fourth session with the consultant, it was established that the dog was actually an assistance animal for Maggie, not just a family pet. The consultant also elicited that when Maggie said Stephen was ‘mean to the dog’ and being ‘tied up’, he was actually tying the dog upside down by its feet and hitting it. Maggie also revealed that this was often in response to Maggie refusing demands for sex, or to get her to agree to sex with the threat of hurting the dog.
This information changed the risk assessment of the level and types of violence against Maggie significantly. Had the consultant not developed the shared communication understanding and taken the extra time with Maggie, she may not have been referred to the appropriate supports needed to recover from her family violence experiences.
Source: Adapted from information provided by Women with Disabilities Victoria.
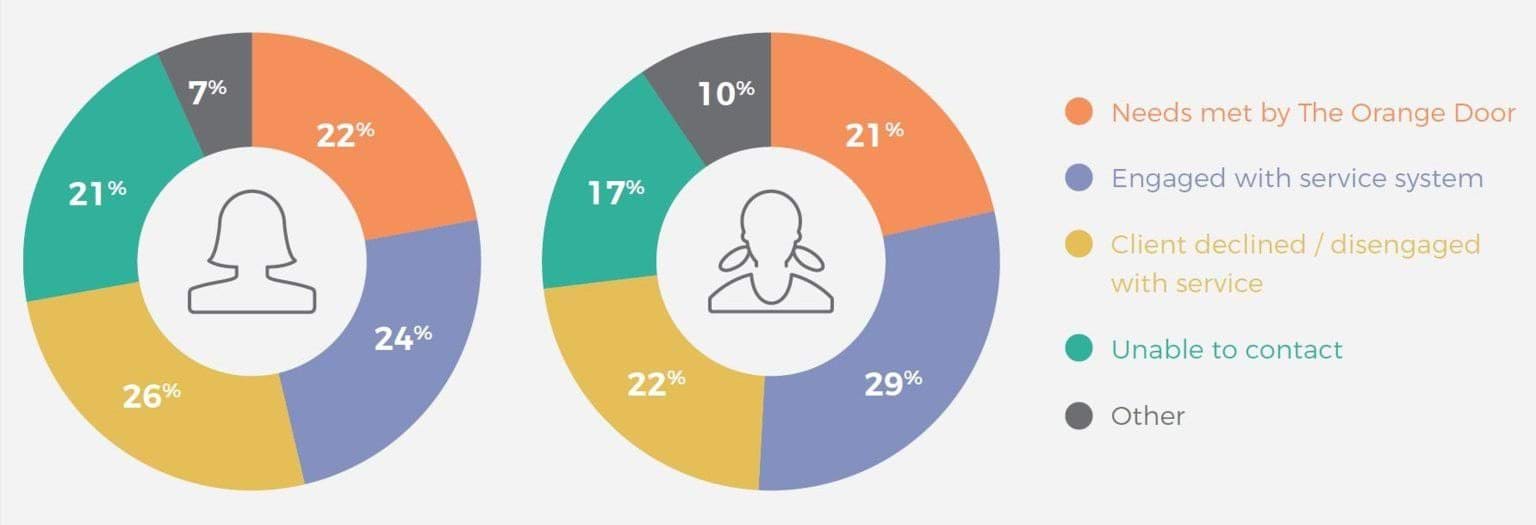
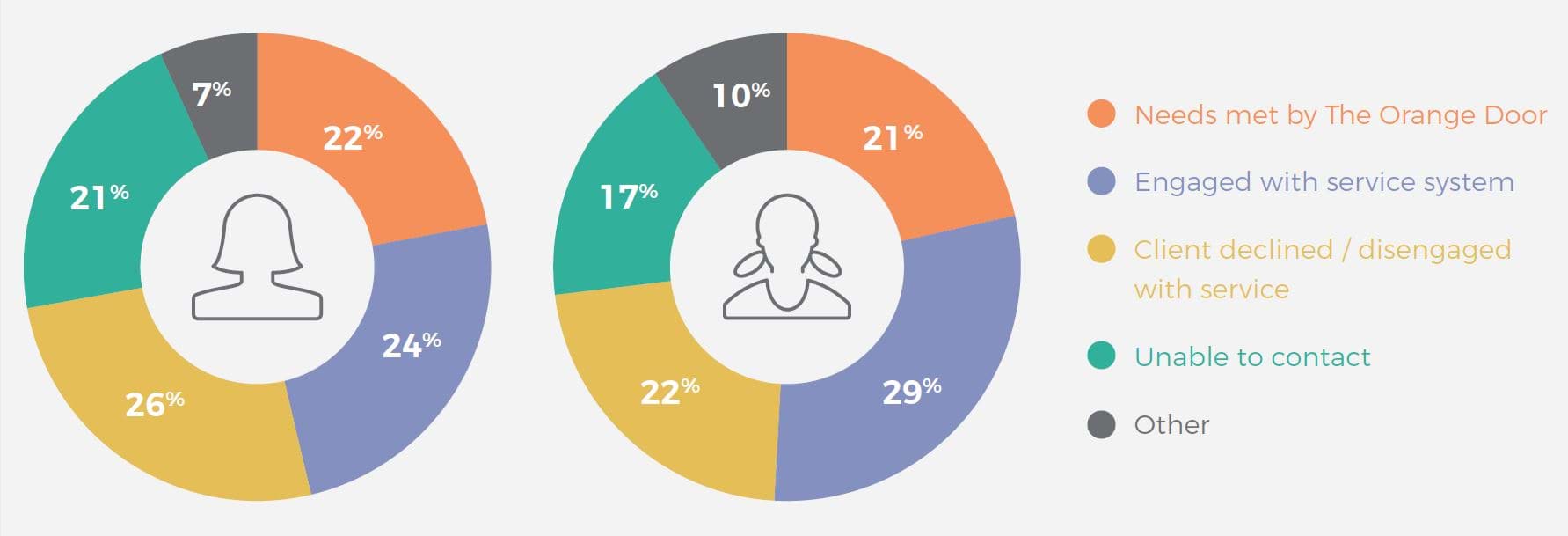
We note that significant proportions of victim survivors are either unable to be contacted or are declining service from The Orange Door (see Figure 7). While acknowledging that The Orange Door is a voluntary service and victim survivors may legitimately choose not to engage, it may be worth exploring this further, particularly the ‘unable to contact’ group.
Figure 7: Victim survivor case closures across The Orange Door locations, by reason
{kind=link}
The implementation of The Orange Door model is an ongoing process, with many sites still very new. As implementation continues, so too must refinement of the model, based on ongoing monitoring. The findings from case file audits will be of great benefit here because they ‘provide insights into the quality of the work that is undertaken with clients and how that work is documented on the case-file’. Systematic case file audits occur three times per year at each site in The Orange Door network. They are carried out by local leadership teams and a findings and recommendations report is prepared and shared with Family Safety Victoria to ensure visibility of issues that may be of system-wide significance. Targeted case file audits can also occur at the discretion of each site’s Hub Leadership Group. While this is an important part of the ongoing monitoring and continuous improvement of practice in The Orange Door, we suggest the following is also required to be able to adequately explore and address the issues we have raised in this section:
- greater central visibility of practice across The Orange Door network by Family Safety Victoria (for example, by establishing an internal review function) [relates to action 16]
- active consideration of timeframes for clients moving through The Orange Door and whether wait times could be improved by streamlining processes [relates to action 14]
- engagement of client voices, including their expectations and experiences of The Orange Door
- analysis of client journeys through The Orange Door and into the service system. Such analysis will be challenging because various parts of the system are using different client management systems, so work to better align these systems over time will also be essential [relates to action 15].
Process for male victim survivors
Of all affected family members (victim survivors) identified by Victoria Police at family violence incidents in 2020–21, 25 per cent were male (22 per cent were males over the age of 18). Notwithstanding the very real issue of some men being misidentified as victim survivors, as explored in our Accurate Identification of the Predominant Aggressor report, there are genuine adult male victim survivors requiring support. Family Safety Victoria has advised that male victim survivors who contact The Orange Door for assistance can be directly supported. Male victim survivors can also contact Safe Steps and receive support, including family violence risk assessment and safety planning in urgent cases. We understand that accommodation options for male victim survivors are very limited, though, and usually rely on the broader homelessness system.
However, in general, adult male victim survivors of family violence have a different pathway into the system. The Victims of Crime Helpline, operated by the Department of Justice and Community Safety, is the main gateway for adult males requiring further support to respond to their experiences of family violence. Male victim survivors identified by Victoria Police through a Family Violence Report are automatically referred to this helpline. Helpline staff can support victim survivors with risk and needs assessments and safety planning, and can refer them on to the Victim Assistance Program (discussed in the next section). Male victim survivors constitute a significant proportion of calls and referrals to the helpline. For example, in 2019–20, 10.7 per cent (1,512) of inbound calls were for male victim survivors of family violence, and 65.7 per cent (17,369) of referrals were from Victoria Police for male victim survivors.
Concerns have been raised about this referral pathway: in particular, that the helpline is a generalist rather than specialist service, and that there is a lack of appropriate referral options. As explained by the Centre for Innovative Justice in its 2020 report on the victim support system:
The current Male L17 Response comprises more than 50 per cent of Helpline referrals but is not supported by a dedicated workforce or specialised response. This is despite recognition among the broader family violence sector that this is highly complex work, including involving predominant aggressor assessments. Further, responding to male victims of family violence represents unique challenges given the lack of services available to this cohort, and the stigma and shame which male victims of family violence may experience.
The centre suggested that, to address this, a dedicated male victim survivor response be established within the helpline to provide more specialised support. It may also be worth considering whether a new pathway to family violence services should be created for adult male victim survivors [relates to action 8]. For example, although The Orange Door and specialist family violence service can and sometimes do support male victim survivors presenting to them, the practice of referring male victim survivors onto a separate referral pathway can create confusion for the public about where to seek support and can come into conflict with the work of the sector to be more LGBTIQ+ inclusive.
Footnotes
- Crime Statistics Agency, Victoria Police Data Tables 2020–21. Table 18: Referrals made by Victoria Police by Police Region and Sex of the Affected Family Member, July 2016 to June 2021
- This is a requirement under the Children, Youth and Families Act 2005.
- Crime Statistics Agency, Victoria Police Data Tables 2020–21. Table 15: Family Incidents Involving Children, July 2016 to June 2021.
- Crime Statistics Agency, Victoria Police Data Tables 2020–21. Table 18: Referrals made by Victoria Police by Police Region and Sex of the Affected Family Member, July 2016 to June 2021.
- For example, Women’s Housing Alliance (2020): Media release: Alliance of women’s housing providers calling for increased funding for the sector, 7 March 2020.
Family violence case management
Demand pressure on family violence services means many victim survivors can’t access the right supports at the right time
After being assessed by Safe Steps and/or The Orange Door, victim survivors can be referred to specialist family violence services for case management support (adult male victim survivors engaging with the Victims of Crime Helpline can be referred to the Victims Assistance Program). Family Safety Victoria has also advised that victim survivors can self-refer to specialist family violence services as part of a ‘no wrong door’ principle. Stakeholders overwhelmingly told us, however, that high levels of demand pressure on the system mean that very few victim survivors will receive case management. We have not been able to obtain any data that describes how many victim survivors are referred to case management, how many receive it, nor how long they wait to commence case management support.
Case management practice
The case management that specialist family violence services provide is now guided by case management program requirements, approved and released in December 2021. The sector was already guided by a code of practice developed by Safe and Equal, which includes practice principles such as person-centred empowerment, inclusion and equity, and child-centred practice. However, the new program requirements represent the first time a case management ‘manual’ has been provided and describe what specialist family violence services need to do to provide high-quality case management services for victim survivors.
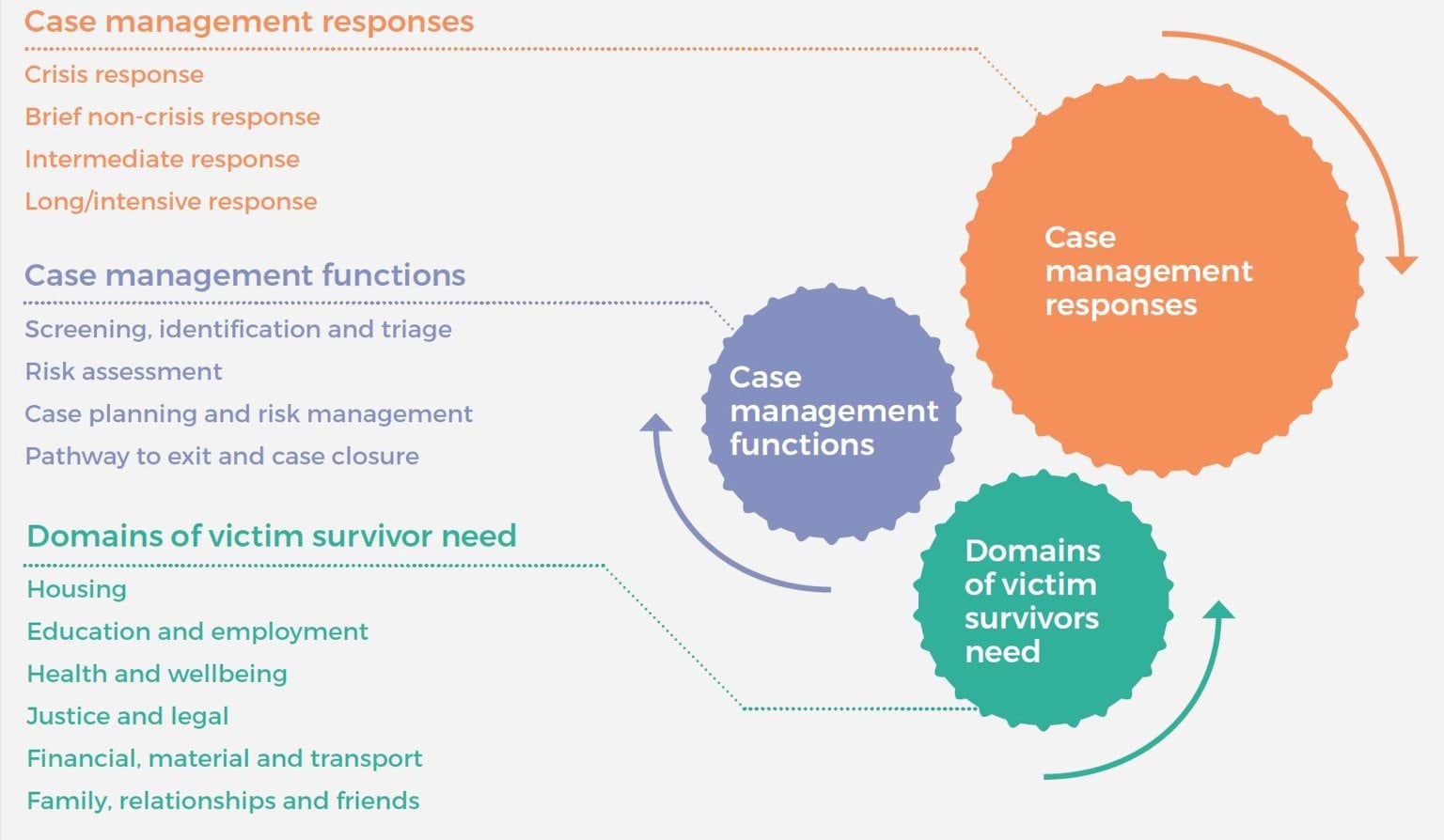
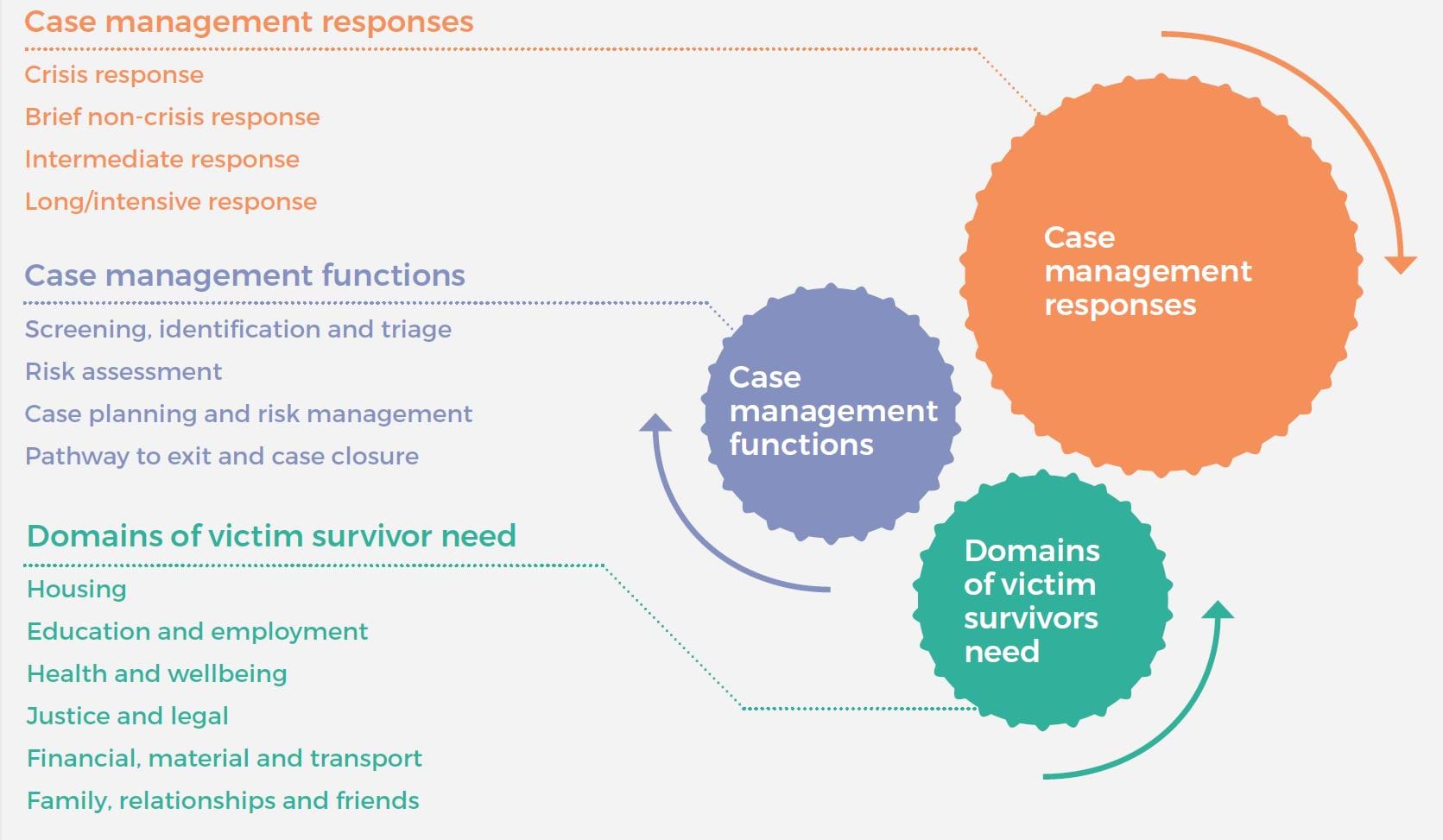
The program requirements clearly outline the types of responses specialist services deliver (from crisis response to a long-term intensive response), the particular functions these services carry out (including risk assessment and case planning) and a series of domains in which victim survivors might need support (including housing and legal). These aspects of case management are outlined in Figure 8.
While there are no timeframes attached to the response types outlined in the program requirements, stakeholders were consistent in telling us that the longest duration of support would normally be three months, with most people receiving around six to eight weeks of case management support. There was concern that three months of case management support for those in the greatest need is insufficient, and anecdotally, case managers feel they are ending their support before victim survivors are ready and able to sustain their own recovery.
It is positive to see the domains of support outlined so clearly in this document, as these reflect the areas of support the Royal Commission explained were essential for victim survivor recovery. Stakeholders, including victim survivors, confirmed this. The challenge, as always, will be to ensure frontline practice reflects the high-level requirements in the context of ongoing demand pressure and workforce challenges. The documentation we reviewed from Family Safety Victoria suggests a gradual process of alignment with the requirements, with support available from Family Safety Victoria and Safe and Equal, and some alignment funding provided to services. Full alignment is expected by the end of 2023. We understand that independent review bodies will examine organisations’ systems, policies and services for their alignment with these requirements as part of broader reviews of compliance with the Human Services Standards. However, we suggest that ongoing monitoring of practice and outcomes, accompanied by appropriate support, will be essential to effectively implement these program requirements.
This ongoing monitoring should consider how different groups in the community are experiencing the service system. For example, there was a perception that victim survivors who wish to remain with the perpetrator will not be supported by specialist family violence services, but the case management program requirements clearly stipulate that such clients are eligible for a brief non-crisis response or an intermediate response.
Figure 8: Program requirements for specialist family violence services
{kind=link}
Family violence case management – supply and demand
Although we have been unable to obtain data on the number of referrals from The Orange Door to specialist family violence services and the wait time to access these services, stakeholders consistently told us about major challenges in connecting victim survivors with services [relates to action 14]. We suggest that without this critical data on referrals and wait times for access, it is impossible for Family Safety Victoria to accurately monitor and model demand for services and plan and allocate resources.
Through recommendation 39, the Royal Commission recommended that:
The Victorian Government, on the basis of demand forecasting, provide sufficient funds to specialist family violence services and Integrated Family Services to allow them to support people referred by a Support and Safety Hub, maintain their safety and help them until their situation has stabilised and they have the support necessary to rebuild and recover from family violence.
Safe and Equal advised us that while specialist family violence services have received large funding increases over recent years, demand is too high for services to be able to meet it [relates to action 13]. It pointed out that enormous investment has gone into creating The Orange Door as the main intake point for the system, but there hasn’t been a sufficient increase in building the service system beyond The Orange Door to ensure a smooth flow of referrals. This means that there are long wait times, leading to people dropping out of the system, or victim survivors’ circumstances changing substantially by the time they connect with a service. This can mean victim survivors have to repeat their story so a new risk assessment can be completed. It can also mean that victim survivors have disengaged from services or are not safe to engage with support by the time a specialist service makes contact with them.
Feedback from the Statewide Family Violence Integration Advisory Committee is that one of the aims of the reform program was to intervene earlier and avoid victim survivors reaching the crisis stage. Consistent with this, the new case management program requirements are clear about the importance of responding to early help-seeking behaviour:
A victim survivor's early help seeking provides a crucial opportunity for preventing an escalation of risk to a serious level of crisis through effective screening, identification and triage, mechanisms for rapid secondary consultations, responsive referral pathways between services and inter-agency partnership …. It is crucial that specialist family violence services recognise and act upon this opportunity when responding to referrals, and especially self-referrals.
Family Safety Victoria has advised that once victim survivors have been assessed at The Orange Door, there are no specific criteria for referral to case management; instead, referrals are said to be based on a discussion with the victim survivor about whether case management is required. Numerous stakeholders told us, however, that in practice only the highest risk clients, and sometimes only those who are considered to be in crisis, are getting through to case management. We heard that case management services previously worked with a greater mix of clients but that their clients are now limited to those at the crisis end, with higher risk and complexity. We understand that in a system under pressure, there is a need to prioritise clients according to need, but we suggest more needs to be done to ensure all victim survivors are getting support to meet their needs and avoid escalation and future incidents, thereby reducing future pressure on the system.
Because of the long wait time for case management support from specialist family violence services, The Orange Door is left ‘holding’ clients, which diverts resources and creates further delays for new referrals.
Stakeholders also shared examples of victim survivors (and risk) being held by a range of other services, many of which are often facing similar demand challenges. For example:
- A maternal and child health family violence worker said she often works outside her scope of work to hold clients facing long (sometimes many months) waits to access specialist services. She does her best to support clients – for example, in applying for an intervention order – but does not feel well trained or supported in doing so. She suggests access to secondary consultations would help her feel more confident supporting clients in this way.
- The Department of Justice and Community Safety advised us that Consumer Affairs Victoria workers are now identifying and assessing risk but are finding that the lower risk referrals are not getting through for specialist support and are therefore left ‘holding the risk’. Many workers still lack confidence in this area, but this confidence is expected to improve as MARAM continues to be rolled out.
- An AOD service provider told us that AOD workers are picking up more of the family violence risk assessment and management that specialist services would otherwise be doing because of the backed-up family violence system. This is said to be placing an extra clinical and emotional burden on AOD staff, leading to burnout.
Sexual Assault Services Victoria advised that with the overall pressure on the family violence response system in Victoria, and imperative to prioritise those at greatest immediate risk, member organisations often struggle to refer victim survivors who are not at immediate risk for family violence counselling and case management. This means that opportunities to reduce risk through early intervention are missed. In addition, we understand that practitioners at The Orange Door are commonly referring to alternative services, even in high-risk cases, because of the demand pressure on specialist family violence services. Such alternative referral pathways include family services and general counselling services. One principal strategic advisor said those services are being flooded with referrals and that they cannot keep up, nor do they have the specialist expertise required. The Department of Justice and Community Safety’s Victims Assistance Program is also increasingly receiving referrals for female victim survivors of family violence from The Orange Door and specialist family violence services. While each Victims Assistance Program provider was recently funded for a position to lead family violence practice due to this increase, the program is designed to be a generalist response for victims of crime.
As suggested in our Early Identification of Family Violence Within Universal Services report, there is a need for a clear model for referral pathways and secondary consultations to support staff in universal health and education services that are encountering clients experiencing family violence [relates to action 1]. This could sensibly extend to other services that are frequently ‘holding’ victim survivors while they await support or directly supporting victim survivors who cannot access specialist services. The model could:
- describe the interface between The Orange Door, specialist family violence services, the Victims Assistance Program and other high-frequency referral points
- clearly outline referral pathways and how decisions about referrals should be made
- clearly outline secondary consultation options
- consider how the needs of particular groups can best be met, such as trans and gender diverse people, and migrant and refugee women, who may find it more difficult to have their needs met by family violence services, particularly in regional areas.
Importantly, consideration must be given to the capacity of services to respond to referrals and secondary consultations.
Stakeholders were clear that the ability for the specialist family violence system to meet demand means that many victim survivors do not receive the type and duration of support they need, and therefore end up cycling back through the system as their situation continues or worsens. We suggest further analysis should be undertaken to determine how boosting the specialist family violence response for more victim survivors would help to reduce overall demand by meeting people’s needs the first time, given the strong feedback we’ve received that many victim survivors are not receiving the support they need until they meet the system’s definition of crisis.
As suggested in the previous chapter, it would be highly beneficial to systematically track victim survivor journeys through the system including referrals, wait times for services, services provided and outcomes [refers to action 15]. We acknowledge that this is currently extremely difficult because each part of the system is tracking data differently and using incompatible information systems [refers to action 14]. In the meantime, we support more targeted, manual analysis of client journeys, including an emphasis on whether or not their needs have been met (as measured against agreed indicators). This will provide a clearer picture of where victim survivors are being referred and their service system experiences.
Victims Assistance Program for adult male victim survivors
As discussed previously, male victim survivors generally have a different service pathway from other victim survivors. After engaging with the Victims of Crime Helpline, they can be referred to the Victims Assistance Program, which is delivered by a selection of agencies in the community such as cohealth and Anglicare Victoria. It provides ‘case management services comprising practical support, criminal justice advocacy and therapeutic interventions to victims of crime throughout Victoria’. However, based on data provided by the Department of Justice and Community Safety, only a very small proportion of males referred to the Victims of Crime Helpline by police end up being referred to the Victims Assistance Program (6.5 per cent in 2019–20; see Table 3).
Table 3: Outcomes of Victims of Crime Helpline contact with males referred by police as Affected Family Members on Family Violence Reports, 2019–20
| Contact action wrap-up | Intimate partner violence | Non-intimate partner violence | Total | Percent (%) |
|---|---|---|---|---|
| Client not reached | 1708 | 1400 | 3126 | 18.0% |
| Client took information for consideration | 1002 | 1044 | 2055 | 11.8% |
| Client declined support | 817 | 1173 | 1996 | 11.5% |
| Client referred to Victim Assistance Program | 503 | 621 | 1129 | 6.5% |
| Client already linked with supports | 323 | 296 | 622 | 3.6% |
| Client referred to other service | 164 | 63 | 227 | 1.3% |
| Other | 3661 | 2168 | 5848 | 33.7% |
| N/A or Missing | 1308 | 844 | 2366 | 13.6% |
| Total | 9486 | 7609 | 17369 | 100.0% |
Source: Department of Justice and Community Safety (2020): Victims of Crime Helpline: Annual Data Report 2019-20.
However, the Victims Assistance Program is generalist in nature. The Centre for Innovative Justice has completed a thorough review of victim services in Victoria, including the Victims Assistance Program, and found that:
Despite a number of skilled and highly dedicated practitioners supporting delivery of the program, and some promising innovations at the local level to meet clients’ needs more effectively, demand pressure on the [Victims Assistance Programs] and a lack of rigorous, outcomes-focussed performance management has resulted in significant variability in terms of the nature and quality of service provision.
To manage high levels of demand, the victims services review found that organisations delivering the Victim Assistance Program were narrowing their service scope and often focusing primarily on practical and criminal justice tasks. They have access to brokerage funding for their clients, and this is primarily used for counselling but can also be used to fund practical and safety supports. These organisations can also contact relevant regional agencies to access Flexible Support Packages for male victim survivors; however, the Department of Justice and Community Safety has advised that, in practice, males are less likely to receive support this way because they will generally be deemed to be at lower risk than female victim survivors.
Some stakeholders told us that the lack of referral options means male victim survivors are sometimes referred to men’s services such as the Men’s Referral Service, Boorndawan Willam Aboriginal Healing Service and Mullum Mullum Indigenous Gathering Place [refers to action 8]. However, these services are designed for men using violence, and the organisations are not funded to work with victim survivors. Boorndawan Willam Aboriginal Healing Service does hold male victims in case management but is concerned that this risks labelling them a perpetrator.
The victim services review called for a more specialised service for male victim survivors, delivering more holistic, needs-based responses. It stated:
As the primary service response for male victims of family violence, [Victims Assistance Programs] need to incorporate a specialised response that more closely reflects supports available to women and children. This includes expanded eligibility criteria to align with legislative definitions of family violence; a greater brokerage allocation to reflect the lack of services, including crisis accommodation, for this cohort; and an appropriate level of specialisation to respond to male victims of family violence, including male children; older men who are victims of elder abuse; and gay, bisexual and transgender men.
Specialist family violence workforce
Workforce challenges are substantially affecting service delivery
A consistent theme across most consultation meetings for this topic was that the family violence sector faces significant workforce challenges, and this is adding to the pressure that services already face due to demand levels and the increasing complexity and severity of cases. This was raised as an issue across The Orange Door, Safe Steps, specialist services and therapeutic services, and we know these challenges extend to other social services. As acknowledged in the Victorian Government’s 10-Year Industry Plan for Family Violence, careful workforce planning is essential to achieve the outcomes articulated in the Victorian Government’s family violence strategies and therefore has a major impact on the victim survivor experience.
The specialist family violence workforce
The 2019 Census of Workforces that Intersect with Family Violence is the most recent source of information about Victoria’s specialist family violence workforce.1 The census showed that practitioners within the specialist family violence workforce (43 per cent of which is located in specialist family violence services) were generally satisfied with their role, the hours they were working and the support provided by their manager. Sixty-one per cent were confident that they had enough training and experience to perform their role effectively.
A range of initiatives have also been put in place to grow the specialist workforce including:
- a dedicated family violence jobs hub and associated recruitment campaign (‘So, what do you do?’)
- the Enhanced Pathways to Family Violence Work Project, where community service and specialist family violence organisations apply to host student placements and introduce students to family violence practice
- establishment of the Family Violence and Sexual Assault Graduate Program and a Family Violence and Sexual Assault Traineeships program.
There have also been initiatives to build leadership capacity within the sector such as the Fast Track intensive leadership program delivered by Safe and Equal, which is free to successful applicants and an important way to improve career pathways within the sector.
However, even pre-COVID-19, there were substantial workforce challenges requiring attention. For example, the census showed that 40 per cent of respondents had plans to leave their current role in the next 12 months. As shown in Figure 9, a significant proportion of respondents cited issues around stress and negative impacts of work as influencing their desire to leave their current role.
Our fourth report to the Victorian Parliament highlighted that retention issues were undermining the significant effort that had gone into workforce attraction and recruitment. As we stated, without dedicated efforts to improve workforce wellbeing and employment conditions, there is a risk of a ‘revolving door’ where ‘people will enter the sector, only to leave through disappointment in workforce resourcing and burn out’.2
Figure 9: Top five reasons for those intending to leave their current position

{kind=link}
During our consultations, multiple sector stakeholders spoke of high levels of workforce fatigue and burnout, resulting in increased absenteeism and turnover and difficulty filling vacancies, in part due to the ongoing impact of COVID-19. These issues are common across the social services sector including for workforces that commonly deliver services to victim survivors such as Child Protection workers and housing and homelessness workers:
Pre-COVID, many community service organisations struggled to secure enough new workers to fill vacancies. Workforce shortages were particularly acute in regional areas. These workforce pressures have been exacerbated by COVID-19, with exponential growth in demand for social assistance. This represents a major existential challenge for the community services industry – and government.
The prolonged nature of the pandemic has left staff stressed and exhausted.
The family violence workforce represents the frontline of reform implementation; it plays a critical role in supporting the recovery of victim survivors and must be supported to do so. The Victorian Council of Social Service highlighted the need to develop strategies that address wellbeing concerns and workforce retention issues by targeting the structural causes of insecure work and low pay in the community sector. We agree, and suggest part of the focus must be on short-term funding arrangements, which stakeholders have repeatedly told us have a significant, negative impact on workforce security and retention [relates to action 9].
There are clearly positive foundations that exist for the family violence workforce, including a commitment to the work and the increasingly professionalisation of the workforce, which many stakeholders highlighted. These could be built upon by ensuring there are ‘career pathways and remuneration that reflects the considerable expertise, risk and complexity specialist practitioners hold’. Given the common issues across social services workforces, it may be worth considering whether the activities designed to attract and retain a diverse workforce within the Child Protection sector could inform activities for the family violence and sexual assault sectors.
Recommendation 209
Numerous stakeholders independently raised the challenge the implementation of the Royal Commission’s recommendation 209 is adding to a workforce that was already struggling. Recommendation 209 is that:
The Victorian Government include in the 10-year industry plan for family violence prevention and response a staged process for the introduction of mandatory qualifications for specialist family violence practitioners, so that no later than 31 December 2020 all funded services must require family violence practitioners to hold a social work or equivalent degree.
The intention of this recommendation was that the introduction of an appropriate minimum tertiary qualification may:
- enhance the professional standing of family violence practitioners
- reflect the range and complexity of their work
- lead to improved remuneration.
This recommendation is now marked as ‘implemented’ on the Victorian Government’s family violence recommendation acquittal website. Implementation has begun through an initial five-year transition period, as described below. From 1 July 2021, any new practitioner within an agency funded by the Victorian Government to deliver family violence services who will be providing specialist services directly to victim survivors and/or perpetrators must meet the Minimum Qualifications Policy pathways to entering specialist family violence work. Key features of the approach include the following:
- Specialist family violence practitioners employed before the start of the transition period are exempted from the minimum qualification requirement, as long as they maintain continuous service in specialist family violence roles.
- New specialist employees have a five-year transition period from 1 July 2021 until 30 June 2026 during which they must either hold a Bachelor of Social Work or equivalent qualification, or be working towards meeting it within five years from their date of employment (if they have at least five years of experience in a relevant field or hold a related qualification).
- Candidates who bring significant cultural knowledge and experience or lived experience and who face barriers to educational pathways can be employed in specialist roles with appropriate support, and have 10 years to work towards a social work or equivalent qualification.
- Employers are responsible for determining whether a candidate’s qualifications collectively meet all seven equivalency principles that have been developed in alignment with the Bachelor of Social Work or whether additional units of learning are required over time to meet the minimum requirements.
The workforce census showed that much of the workforce already holds a qualification of some sort (most frequently a bachelor’s degree – 49 per cent of census respondents held a qualification of this type), so it seems that many new specialists are likely to have at least met some of the equivalency principles.
Most stakeholders who expressed concern about the requirements spoke about the social work degree in particular; they didn’t feel it was essential for the job and felt very limited in who they could hire. Aboriginal Community Controlled Organisations, in particular, felt that the policy insufficiently acknowledged lived experience and on-the-job training. Safe and Equal, which is directly supporting services to implement the policy, has advised us that the policy can be difficult for family violence services to implement. They said there is variability in the level of understanding of what ‘equivalent qualifications’ means and that employers can be fearful of ‘getting it wrong’, which leads them to narrowly interpret the policy as a requirement for applicants to have a social work degree.
These challenges were directly acknowledged in advice released by the Department of Families, Fairness and Housing in September 2022. This advice recognised that ‘these ongoing challenges mean that not all practitioners will be able to be hired in precise accordance with the Policy pathways at this early stage of implementation’. It emphasised that:
The Policy puts employers at the centre of determining if a candidate is the right fit for the role and meets an employment pathway under the Policy. Expectations of the shift to meeting the Policy are of progressive change and we want to avoid the Policy driving unintended consequences.
This advice may help to build the sector’s confidence to implement the policy more fully, and this will continue to be monitored through the Transition Monitoring Advisory Group. Acknowledging that a review of the policy will occur during the transition period to determine whether any changes are required, we suggest further consideration of:
- how the policy intersects with the Social Services Jobs Guarantee, which matches Diploma of Community Services graduates with jobs in a range of social services including family violence and sexual assault services
- the additional guidance and resources required for organisations recruiting candidates on the lived experience pathway [relates to action 10]
- whether organisations need additional support to map relevant past experiences and qualifications and determine appropriate pathways to meet the equivalency principles.
Lived experience workforce
Victim survivors we met with spoke about the healing power of supporting and/or advocating for other victim survivors by engaging in lived experience work in the sector. For example:
Becoming a Survivor Advocate has helped me to rise above fear, doubt and mental health issues and recover from my experiences. It has been so rewarding getting to meet so many other survivors who are all such inspirational, courageous women.
The industry plan notes the importance of the voices of victim survivors being strong throughout the family violence system. It commits to ‘creating genuine employment opportunities in specialist family violence and primary prevention organisations’ and recognises that:
Victim survivors working in these fields need a range of professional skills to complement their lived experience. Family violence doesn’t discriminate and victim survivors possess a great diversity of skills, knowledge and experience across a range of disciplines, so skills support needs to be provided on a tailored basis, based on an assessment of each individual’s needs.
Some stakeholders pointed out there is currently no model or career pathway for a lived experience workforce in the family violence sector. We note that the Mandatory Qualifications Policy provides a dedicated pathway for people with lived experience to enter the specialist family violence workforce. However, there is no specific framework around lived experience work, as there is in the mental health sector.
The mental health sector has seen government investment in lived experience roles, including peer support positions. This is expected to grow as the system and services reorient to meet the directions of the Royal Commission in Victoria’s Mental Health System, which places lived experience at the centre of reform including lived experience leadership at every level. The Victorian Council of Social Service has suggested that government ‘leverage insights from the mental health reforms to develop strategies to encourage people with lived experience to become community services industry employees and to support them in their roles’.
Victoria’s new mental health and wellbeing workforce strategy positions lived experience as ‘central to the transformation of the mental health and wellbeing system’ and includes 10 priority actions to develop and embed the lived experience workforce. These actions are about establishing new roles, training and development, access to supervision, career pathways, and attraction, recruitment and retention. The strategy highlights a $40.7 million investment into lived experience workforces ‘to support and grow the consumer and carer lived experience workforces, including support for 30 peer cadets each year’. Examples of lived experience roles in mental health settings are listed at Figure 10 and could inform the types of lived experience positions that the family violence sector could benefit from.
Figure 10: Examples of specific lived experience roles across role categories in mental health settings
| Peer support workers |
Consultants | Managers | Educators | Advocates | Researchers |
|---|---|---|---|---|---|
| Consumer peer support workers use their personal lived experience of mental illness and recovery to support other consumers individually or in groups. | Consumer consultants collate information and feedback from consumers about their views and experiences of a service and use this information to make recommendations for service improvement. | Lived experience managers are experienced consumer or family/carer workers who support and develop other lived experience workers. They may or may not line-manage staff or provide practice supervision for, or mentor, other workers. | Consumer and family/carer educators ensure consumer and family/carer perspectives, participation and involvement are included in all aspects of education and training provided in services. | Consumer advocates support consumers to have a voice and be a party to issues that affect them; Carer advocates support family/carers to be heard in relation to issues that affect them. | Consumer and carer researchers draw on their lived experience to promote and enable the engagement of consumers and carers at all stages of research. |
Source: Department of Health (2021): Lived experience workforce positions report: Victorian mental health and alcohol and other drug services 2019–20, pp. 8-9.
There are clearly some challenges in building and maintaining this workforce. For example, the lived experience workforce in mental health has a vacancy rate of 23 per cent, the highest vacancy rates of all public specialist mental health services workforces. Feedback from the Department of Health is that formally introducing an effective lived experience workforce takes many years and that it is most important to ensure:
- lived experience workers have role clarity
- employers and colleagues understand the role of lived experience workers
- employers and colleagues create the conditions that allow lived experience workers to thrive.
We suggest any work to formalise a family violence lived experience workforce should prioritise these fundamental areas and consider the applicability of other features of the mental health lived experience sector [relates to action 11]. These include:
- the existence of a Certificate IV in Mental Health Peer Work
- the launch of the Lived Experience Peer Cadet Program for those undertaking the qualification
- the development of a suite of resources to support employers, including a self-assessment tool to measure an organisation’s maturity in being able to support lived experience practitioners.
Furthermore, Family Safety Victoria’s Family Violence Lived Experience Strategy contains principles co‑designed by the Victim Survivors’ Advisory Council, as well as lessons learned from the council’s model, which may support the formalisation of a lived experience workforce in the sector.
Footnotes
- We note that a family violence and sexual assault workforce pulse survey was carried out in September and October 2022, but the findings were not available for this report.
- Fenton (2019): Family Safety Victoria: Research to Inform the Development of a Campaign to Grow the Family Violence Workforce, p. 6.
Navigating the service system
Navigating the family violence and related systems remains a challenge for victim survivors, but there are some good examples of coordination
As acknowledged in the new case management program requirements, victim survivors may need support across a range of domains, spanning:
- housing
- education and employment
- health and wellbeing
- justice and legal
- financial, material and transport
- family, social and community connections.
Based on our consultations, it is very difficult for victim survivors to navigate the range of systems they need or are required to engage with. A victim survivor also explained how interrelated their needs can be, saying that:
… you need housing to even think about looking for a job, but if you don’t have money, you can’t get housing – you get stuck in this loop.
There is some good local practice that aims to support victim survivors in a more holistic and joined-up way to meet their needs, but this is not supported systemically due to narrow funding streams and reporting requirements.
Service system navigators
Following the Royal Commission, and in response to victim survivors saying they wanted someone to help guide them through the system, the Victorian Government stated through its 10-year family violence plan that:
Victim survivors will not have to navigate the complex legal and community services systems by themselves. Service navigators will be highly skilled specialist workers that will have the flexibility and capacity to support people from crisis through to recovery, and ensure they are supported in a simple, timely and coordinated way that works for them.
It acknowledged that there are highly skilled case managers providing this kind of support, but there are not enough of them and ‘funding and program constraints … get in the way of providing the support women and children need’. Service navigators were intended to be highly skilled specialist workers who could support women and children from crisis through to recovery, working in strong collaboration across community and justice services [relates to action 12].
“Ultimately, every case of family violence needs a qualified case worker with the ability to work with the survivor in navigating their path away from violence, including an authority to act (where survivors have given consent) to enable the case worker to ‘do’ some of the work and lighten the survivor’s unrealistic and unbearable load."
Lily, victim survivor
While service system navigator positions do exist in The Orange Door model, they are more strategically focused on service pathways within the local area and not the direct client support roles as envisioned in the 10-year plan. While there may have been pragmatic reasons to make these roles more strategic, victim survivors still see the need for practical, guiding support, and other stakeholders reiterated that the system remains difficult to navigate. For example, the Statewide Family Violence Integration Advisory Committee noted in an internal presentation that ‘our service system is complex and opaque, especially to service users. Clients should not be made responsible for navigating this complexity when they need our services.’ Similarly, a community legal centre told us that ‘navigating the service delivery system is a full-time job in itself, (and) putting (that) responsibility on the victim survivor is not right’.
Victim survivors spoke of not being able to think clearly when trying to get themselves out of a family violence situation. They noted that they are often provided with information about where to go for support but don’t necessarily have the headspace to pursue these things on their own. They wanted help with the ‘doing’, such as engaging with Centrelink.
We suggest there must be clarity around whose role it is to lead coordination and navigation work for a victim survivor, whether practitioners at The Orange Door or case managers at specialist family violence services or others.
“Peer support is often the best support. Victim-survivors have a different way of ‘knowing’ and understanding what their peers are navigating."
Lily, victim survivor
Building on the discussion from the previous chapter about strengthening a lived experience workforce in the family violence sector, there may be the opportunity for lived experience practitioners to support victim survivors with system navigation.
“With fellow survivors/peer supports, frustrations and feelings can be heard without judgement but can also help guide survivors through the system."
Kelly, victim survivor
Specific navigation challenges for victim survivors
The challenges victim survivors face in navigating the service system can relate to the sheer number of services required, the various eligibility criteria they may need to meet and the range of processes for accessing services. It can also relate to the limited capacity of services, resulting in victim survivors facing long waitlists and unsure where to turn next (specific capacity issues across services are discussed in the next chapter). Some systems, though, were raised as not adequately responding to family violence, and which are substantially affecting their recovery. These are discussed below.
Child Protection
Stakeholders have consistently raised their concerns about Child Protection practices in respect to responding to family violence over recent years. The Commission for Children and Young People advised us that family violence continues to be a common theme in the child death inquiries it conducts for children who were known to Child Protection in the 12 months prior to their death. It also advised that it continues to see evidence in Child Protection responses of inadequate understanding of the impact of family violence on children, inadequate assessment of family violence risk to children, and that sufficient safeguards and supports are not always being put in place for child victim survivors or their families (including adult victim survivors and perpetrators), particularly at the point of case closure. This can mean children (and protective parents) continue to face family violence risk, often resulting in further reports to Child Protection. This is a major barrier to recovery, especially when children and families are not linked to therapeutic supports.
We recognise the complexity of child protection work and the substantial efforts made to support this demanding area. Stakeholders said Child Protection policies are strong on paper but are not necessarily implemented consistently on the ground. This aligns with what we previously found in our fourth report to parliament and our Accurate Identification of the Predominant Aggressor report. We acknowledge the dedicated, ongoing work of the Department of Families, Fairness and Housing to improve the family violence capability of the Child Protection workforce and the workforce challenges this sector faces. This report doesn’t explore Child Protection practice in detail, but stakeholders have repeatedly expressed what they perceive as key issues with Child Protection practice, including:
- the need for a stronger focus on holding the person using violence to account rather than the protective parent
- protective parents (usually women) being expected to leave a relationship in order to keep their children
- the need for further work to align with MARAM.
Stakeholders provided a range of examples emphasising the need for the Child Protection workforce to improve its understanding of the complexities of family violence dynamics and improve the way this understanding is used to drive decision making and practice.
Victoria Legal Aid said that Child Protection frequently recommends withdrawing protection applications on the condition that women make a family law application. It highlighted that, particularly because there is no guarantee that the family law outcome will limit or prevent contact with the perpetrator, this can be counterproductive and exacerbate family violence risk if the perpetrator had not been pursuing contact with the children.
Women’s Legal Service Victoria raised concerns about inadequate support for mothers whose children are permanently removed, or temporarily removed and then returned. For example, Child Protection is no longer involved once a child is returned to parental care, yet there is no system-wide response to ensure the family receives the ongoing, integrated support needed to address the underlying issues. Similarly, the Statewide Family Violence Integration Advisory Committee suggested the need for improved referrals to family violence services, with Child Protection at times encouraging women to self-refer into family violence counselling when they clearly require case management.
While early legal advice is vital for all victim survivors, particularly where Child Protection has become involved, it was raised as essential for Aboriginal victim survivors, given the history of over-representation of Aboriginal children in out-of-home care. Where victim survivors of family violence are seeking specialist family violence support and also navigating the Child Protection system, they need to be supported with culturally appropriate services and legal advice. We were told that without this, the confidence of Aboriginal mothers to report family violence and access the services they need to keep themselves and their children safe will be diminished. Djirra has proposed a notification system whereby an Aboriginal service is directly notified when a report to Child Protection involves an Aboriginal child, to help activate early legal assistance. The Department of Families, Fairness and Housing has advised that this idea has been explored previously and has been found to be unfeasible. It pointed to existing safeguards, such as a requirement to consult with the Aboriginal Child Specialist Advice and Support Service regarding decisions for Aboriginal children, and the provision of legal support at the Children’s Court of Victoria, where Child Protection matters are heard. We are unable to comment on the sufficiency of these safeguards or the feasibility of Djirra's proposed notification system, but we encourage ongoing work between the Department of Families, Fairness and Housing and Aboriginal Community Controlled Organisations to ensure Aboriginal families can more easily access the range of services they need.
Commonwealth Government systems
While Commonwealth efforts go beyond the scope of our analysis, we cannot ignore the numerous stakeholders, including victim survivors, who passionately told us about the need for improvement in a range of spaces for which the Australian Government has direct responsibility. These spaces particularly include:
- the family law system
- the immigration system, and temporary visas
- income support through Centrelink.
The Victorian Government urged the Australian Government to specify and call out what action will be taken for women vulnerable to victimisation because of their visa status, such as women on temporary visas. It suggested there needs to be structural reform of the legal, migration and welfare systems to ensure women and children on the full range of temporary visas who are at risk of or have experienced family or sexual violence have access to the supports they need. Similarly, Safe and Equal called for action around immigration laws and eligibility criteria to ensure women and children on temporary visas can access appropriate supports, including through Medicare. It also called for:
- ‘increasing income support payment levels to improve women’s economic security and ability to leave relationships without being at risk of poverty.
- holistic reform of the family law system to ensure safety of victim-survivors is prioritised and to reduce opportunities for systems abuse.’
[In family law matters] "...a father’s right to parent trumps everything else – it’s the one area where we’re going backwards."
Jess, victim survivor
Issues around the family law system were very frequently raised during our consultations as being major barriers to recovery. There was some acknowledgement by legal services that family law courts are gradually improving. But victim survivors were particularly clear about the trauma of having to regularly hand children over to their perpetrator over many years as a result of a parenting order being made by the Federal Circuit and Family Court of Australia. Victim survivors in this situation are fearful for their children’s safety and wellbeing and are often themselves subjected to ongoing emotional and systems abuses at the hands of the perpetrator.
"When a survivor is forced to share parenting with a perpetrator, it is near impossible to recover. Perpetrators do not co-parent, they counter-parent. Survivors need ongoing, long-term supports in navigating endless coercively controlling behaviour."
Lily, victim survivor
The National Plan to End Violence Against Women and Children 2022–2032 acknowledges some of these issues. It commits to acting on the recommendations made by two recent reviews of the family law system to make it safer and easier to use and to ensure safer outcomes for women and children. It acknowledges the need to ‘break down the systemic barriers that directly impact women from migrant and refugee backgrounds’. We also note that the national Meeting of Attorneys-General Family Violence Working Group, formed in 2017, is ‘developing measures to improve the interaction between the family law, child protection and family violence systems’.
We encourage the Australian Government to pursue strong action in these areas, focusing on improving victim survivor experiences of these systems. We also suggest further consideration of whether Centrelink processes could be improved, as victim survivors commonly identified Centrelink as being difficult to navigate and a source of stress during times of crisis [relates to action 4].
Importance of service coordination
Victim survivors’ range of needs and challenges are highly inter-related, and many stakeholders spoke about the interconnectedness of family violence, mental health and AOD issues, in particular. The value of a coordinated approach seems self-evident; however, we understand that services are usually not well coordinated. We commonly received feedback that funding is siloed and service requirements can be very narrow, and that these can be barriers to organisations providing more holistic victim survivor responses. Additionally, Aboriginal family violence services are known to provide holistic responses, working with whole families to address their wide-ranging needs; however, Aboriginal Community Controlled Organisations commonly raised short-term and insufficient funding as a barrier to strong, community-led service delivery [relates to action 12].
The Statewide Family Violence Integration Advisory Committee spoke about a lack of coordination between the mental health, AOD, housing and family violence systems. They said that each of these systems is often overwhelmed with demand, so if one service opens a case for a victim survivor, the others will close theirs, unless it is an exceptionally high-risk case.
The specialist family violence capacity-building roles located within mental health and AOD services were very highly regarded and were seen to be improving the way these services respond to family violence. However, due to a lack of clarity and embedded practice around collaboration, information sharing and secondary consultation across service systems, an unintended consequence was said to be that these services are less likely to reach out to specialist family violence services and more likely to rely on their internal specialist role, leading to further siloing between systems [relates to action 1].
Stakeholders raised various examples of the need for further co-location of services to improve the way victim survivor needs are identified and met [relates to action 2]. One duty lawyer at a specialist family violence court said that having, for example, a practitioner from inTouch Multicultural Centre Against Family Violence or The Orange Door in court was a highly effective way to directly connect the victim survivor with support. Since COVID-19, however, we understand some of this co-location in court has been lost. Another suggestion is that financial and legal support should be integrated into The Orange Door service model to ensure victim survivors can get prompt advice and support to prevent legal and financial damage from accruing [relates to action 5]. We are aware that legal services are being piloted at one of The Orange Door locations and suggest a broader rollout based on lessons from the pilot is seriously considered.
Mechanisms for greater coordination are needed to ensure victim survivors’ needs are being met. These could include:
- a clear model around secondary consultation, collaboration and referrals
- increased use of the Family Violence Information Sharing Scheme to better coordinate services for victim survivors and reduce the need for them to re-tell their story
- increased co-location of services.
We also note some existing enablers of coordination and good local practice to provide more holistic responses.
Over recent years, stakeholders have consistently told us about the value of Family Violence Flexible Support Packages (FSPs) in being able to promptly provide tailored support to meet the needs of victim survivors. This is one way more coordinated and victim-centred support can be provided. FSPs aim to support a victim survivor’s safety and security, health and wellbeing, capabilities to participate, and connections to community and culture. Their use ‘must represent the most cost-effective, timely and appropriate response to meet the outcomes identified in a victim survivor’s case management/support plan’. Some of the supports allowed are represented in Figure 11. While the maximum allowed FSP is $10,000 for a support period, the average cost of an FSP is $3,400. To be eligible for an FSP, the victim survivor must have left the perpetrator, be planning to leave or have the perpetrator removed from the home, although an exception is made for Aboriginal victim survivors. Where a victim survivor is still living with the person using violence, the focus must be on ‘responses that will minimise risk to victim survivors, ensuring that responses do not escalate, reward or reinforce abusive behaviours’.
Figure 11: Possible uses of Flexible Support Packages

{kind=link}
Organisations we met with that deliver multiple services spoke of the profound benefit of being able to easily connect a victim survivor with the services they need within the one organisation. Organisations like The Salvation Army, Nexus Primary Health, VincentCare, Mallee Family Care and many Aboriginal Community Controlled Organisations all offer some combination of services such as specialist family violence services, financial counselling, legal support, homelessness services, AOD support, disaster and emergency relief, employment services and counselling, among others. See Box 3 for one example.
Box 3: An integrated service response from McAuley Community Services for Women
Following a two-week stay in a McAuley refuge, Julia and her three children were transferred to McAuley’s supported accommodation. McAuley case workers supported Julia and her children in identifying their priorities, individual needs and lasting solutions to individual goals. Julia and her children also accessed the onsite counselling services.
Julia’s children’s needs were assessed and resulted in liaison with a National Disability Insurance Scheme worker to secure support for one child. A school pack was provided to a primary school–aged child and toys provided for all the children. They also received material aid including bed linen, pyjamas and food vouchers.
Through McAuley Works, Julia was supported into employment. She started her new job four months after being referred into McAuley Works.
Julia was also referred to WEstJustice through McAuley’s partnership and received legal advice to support her situation.
Transitional housing was offered, but Julia declined this, instead finding rental accommodation on her own. Working with another service provider, McAuley ensured the cost of moving house was covered and that there was adequate furniture. McAuley also worked with Julia to ensure a comprehensive safety plan was put in place, including emergency contacts and processes.
Both Julia and one of her children were connected to specialist counselling services to support them following their interaction with McAuley.
While Julia was not ready to join a community group at the time, McAuley provided Julia with resources to support her linking in with her new community when she is ready.
The integrated service model allowed Julia to move safely to a new home, identify a new income source through employment and link with new legal and counselling services, all while reducing the impact on her three children.
Source: Based on a case study from the 2021 McAuley Community Services for Women Annual Evaluation Report.
There are also promising examples of regional efforts to integrate local practice. One example is the Ovens Murray Integrated Response Panel, which was created as part of a broader regional effort to increase systemic coordination between the family violence, AOD and mental health sectors within the Ovens Murray catchment. The panel applies a collaborative approach to achieve better outcomes for clients who have cross-sector needs. The monthly panel consists of case managers from agencies within the family violence, mental health and AOD sectors. Senior staff from Child Protection and Albury Wodonga Aboriginal Health Service also attend where required. With the consent of the victim survivor, a case can be presented to the panel to generate joint responses to complex cases that have not been improved by initial interventions. It also improves cross-sectoral connections and clarifies referral pathways for practitioners. The initiative was evaluated in 2021, demonstrating clear value and potential as a forum for facilitating cross-sector practice discussions for complex cases. Through the evaluation, practitioners advised that the panel provides a space for different services to share their expertise and interpretation of the presenting issues to inform case planning, and encourages collaborative and client-centred practice. However, the evaluation identified that refinements were needed to address low referral numbers and to further enhance outcomes. An example of a case supported by the panel is provided in Box 4.
Box 4: Ovens Murray Integrated Response Panel
Vicky is a 37-year-old female enrolled in a 12-month AOD recovery program and family violence counselling.
Vicky experienced a highly traumatic and stressful period, including the death of a child and a new relationship with a family violence perpetrator who bought her alcohol, but she remained engaged with services. Over this stressful period, a referral had been made to a mental health service, but service had not begun.
Vicky tried to take her life and was in hospital when she contacted her AOD worker. It seemed she would be discharged to her home where the perpetrator was still living and where she faced an ongoing family violence and alcohol abuse risk.
A shared system response was needed and so Vicky consented to a referral to the Ovens Murray Integrated Response Panel. Using the panel structure, case managers from the family violence, AOD and mental health sectors were able to:
- use clear and timely communication about the current situation, risks and safety
- identify a rapid response to use the mental health system to support Vicky through an admission that also made time for court processes (to seek a family violence intervention order)
- facilitate the removal of the perpetrator from her home and activate other safety measures before she was released from hospital
- use the space to advocate for Vicky’s needs by sharing information, which supported a shared understanding of her situation and collaborative work.
Vicky has remained engaged and supported. Practitioners report that, having used the panel, benefits continue as they all work together to meet Vicky’s needs.
Source: Based on a case study in Ovens Murray Family Violence Capacity Building Project, Evaluation Report (January 2021).
Reforms underway that respond to recommendations from the Royal Commission into Victoria’s Mental Health System may also support improved cross-sector collaboration and coordination. For example, it recommended establishing Regional Multi-agency Panels. These panels’ membership and functions aim to support better cross-sector coordination, collaboration and accountability between the mental health service systems and other sectors, which could include family violence services.
Range of support services
Victim survivors are accessing a range of systems and services that often struggle to keep pace with demand
As established in the previous chapter, the range of services victim survivors need are often not well coordinated and can be very difficult to navigate. This chapter goes into further detail about four types of support that are critical for victim survivor recovery but that often struggle to keep pace with demand and to reach victim survivors:
- housing assistance
- financial support
- legal and court supports
- therapeutic services.
Housing assistance
As one stakeholder explained, without somewhere consistent to live, it is virtually impossible to get back on track. As well as being a fundamental need, stable housing is also inextricably linked to employment, income support and financial independence. The Royal Commission was clear about the importance of victim survivors being able to access safe, stable and affordable housing:
A lack of housing options can exacerbate the trauma and dislocation of the violence, disrupting social and economic participation and education and adversely affecting health and wellbeing. In some cases it forces women to choose to return to a violent partner. Once women and children who have experienced such violence are housed in a safe place, they can begin to rebuild their lives and plan for the future.
There is a clear relationship between family violence and homelessness, with the Australian Institute of Health and Welfare identifying that of clients commencing support with a homelessness service in Victoria in 2020–21, approximately 47 per cent identified family violence as a reason for seeking support.
We looked closely at this issue as part of our fourth report to parliament. We found there were chronic housing shortages, particularly in the availability of social and affordable housing, and that it was often very difficult for victim survivors to safely remain in their own homes. We found that these housing shortages were creating major blockages for victim survivors trying to move from crisis towards recovery and stability.
There have been major investments in social and affordable housing in recent years. For example:
- The $5.3 billion Big Housing Build, announced in 2020, includes delivery of 9,300 new social housing homes (up to 1,000 of which are for victim survivors of family violence) and $50 million for new housing projects for young people experiencing or at risk of experiencing homelessness.
- As part of a COVID-19 housing economic stimulus package, $500 million was directed to building and upgrading more than 23,000 social housing dwellings; $10 million of this is to increase support options for women and children escaping family violence.
- Through both the From Homelessness to a Home program and the Homes for Families investment, approximately $232 million has been provided to help move people living in emergency hotel accommodation due to COVID-19 into long-term stable housing.
Based on our consultations, we understand that these issues remain; when we asked stakeholders to identify the main areas for system improvement to support victim survivor recovery, they very commonly raised housing. Figure 12 depicts some of the ongoing shortages of housing support for all clients (including victim survivors), with glaring gaps in the availability of long-term housing for those who need it.
Figure 12: Clients need for accommodation services and proportion where housing support was provided to meet these needs, 2020-21, Victoria

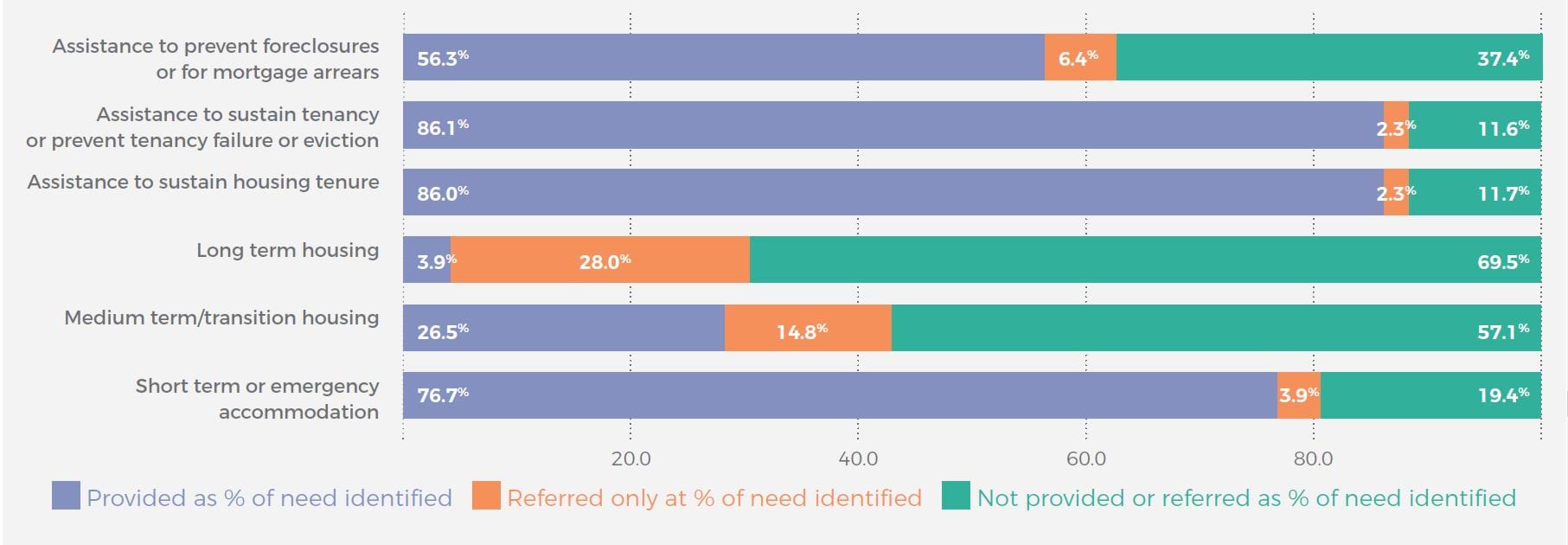{kind=link}
While not all victim survivors need social housing, for some it may be the only way for them to achieve long-term housing stability. Social housing bottlenecks also create upstream bottlenecks in crisis accommodation and refuge. As shown in Figure 13, there is far greater demand for social housing than can be met, with only about 10 per cent of applicants on the Victorian Housing Register being allocated social housing in a given year.1 Victim survivors of family violence face an average wait time of 17 months to access social housing.
Figure 13: Applications, allocations and wait time for social housing in Victoria
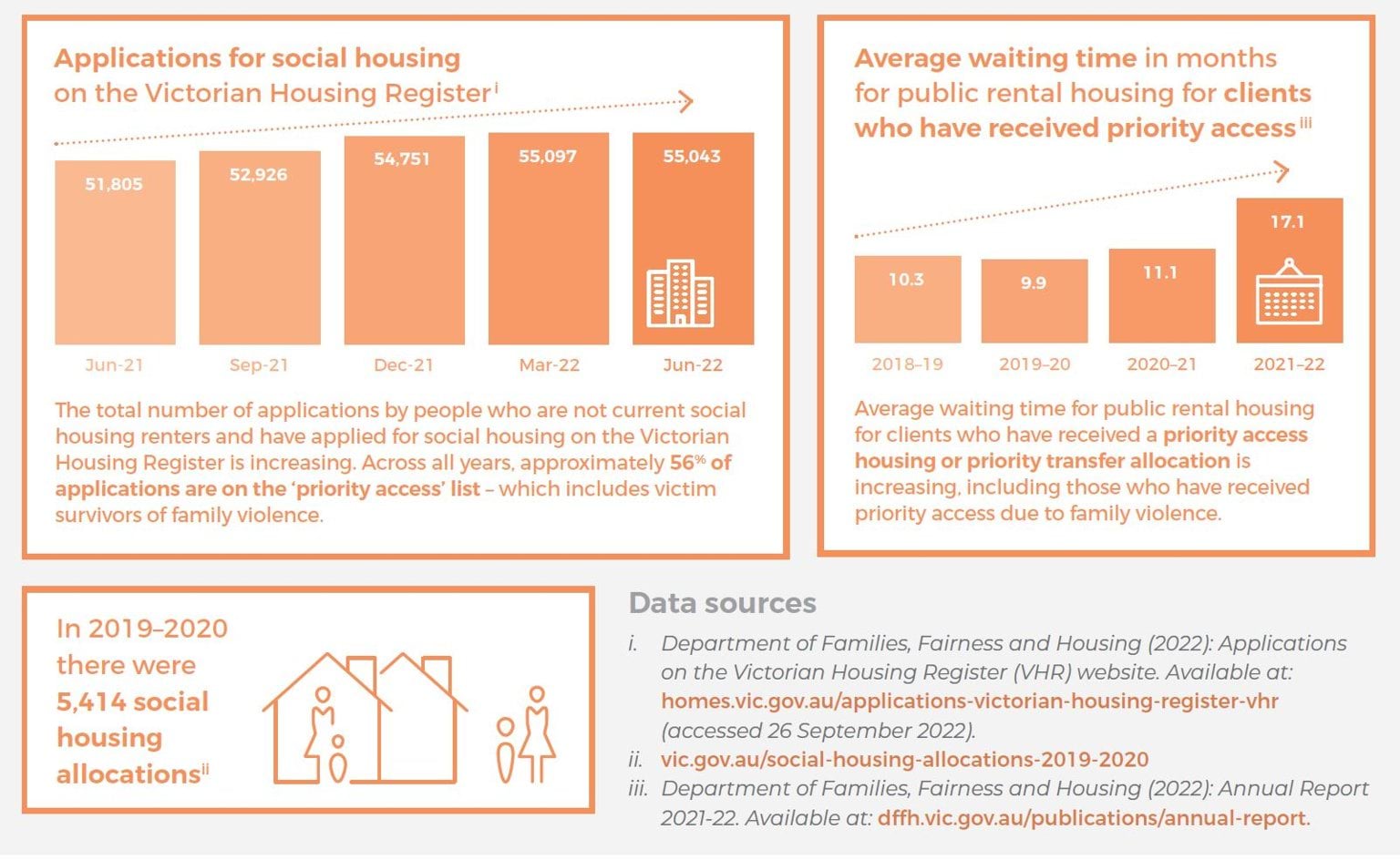
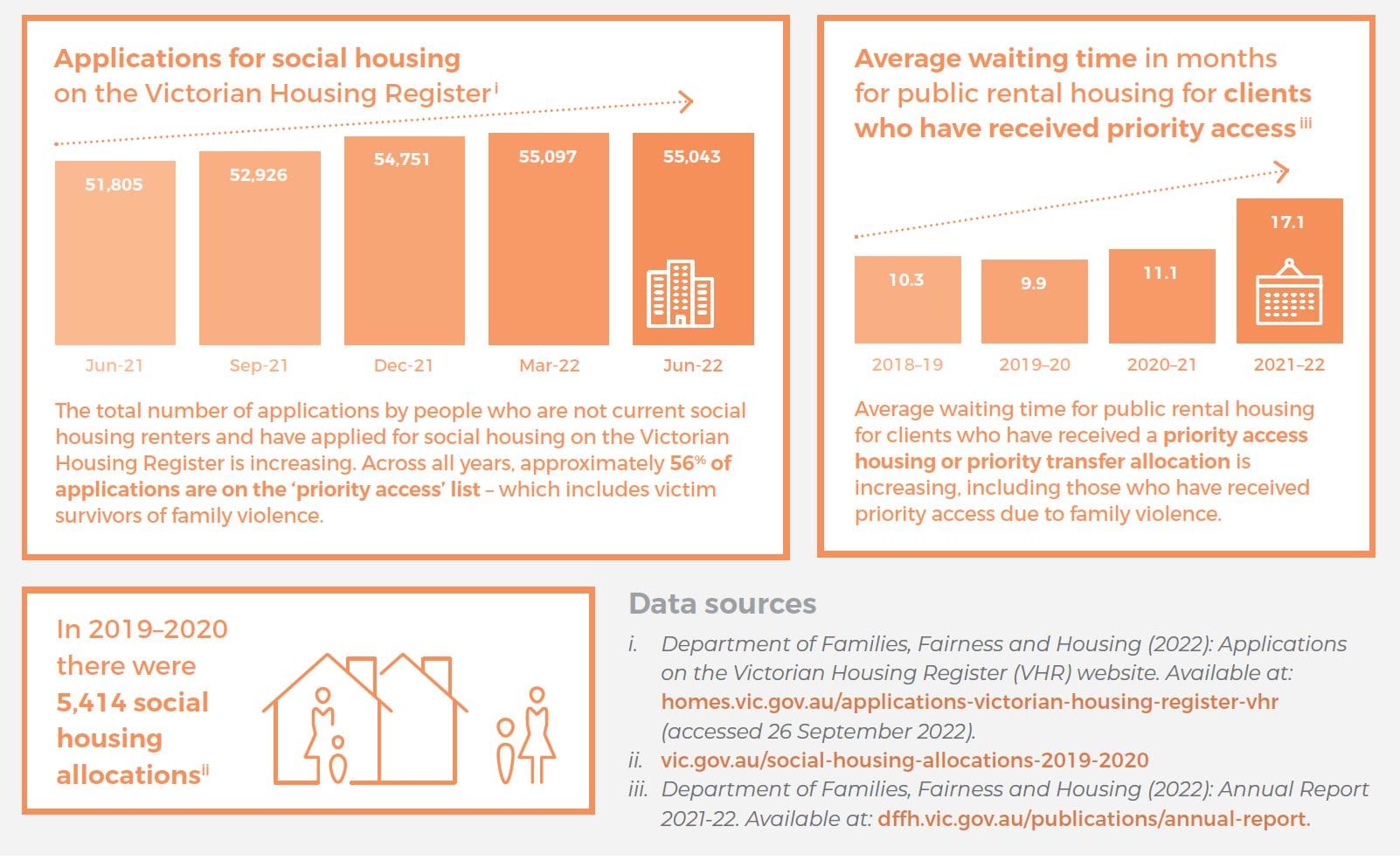{kind=link}
We echo what is stated in the Establishing a 10 Year Strategy for Social and Affordable Housing discussion paper:
A fundamental step change in policy and delivery is needed to embed the foundations for growth and sustainability of social and affordable housing in Victoria … the social and affordable housing challenge will require ongoing effort over many years, extending beyond the Big Housing Build.
Given the seemingly intractable housing issues that remain, we can only encourage ongoing investment across the housing spectrum from crisis to long-term social and affordable housing, and the pursuit of other options to support victim survivors to maintain rent and mortgages [relates to action 13].
"The scariest thing about leaving or preparing to leave is not having somewhere to go. Homelessness services are underfunded … so people are faced with either returning to unsafe situations or sleeping rough either by themselves or with children."
Kelly, victim survivor
Financial support
Through consultations with stakeholders such as the Department of Justice and Community Safety, Financial Counselling Victoria and the Economic Abuse Reference Group, we were struck by how important it is that victim survivors have access to support that promotes their economic security, in the context of a range of forms of financial abuse that victim survivors are experiencing. Some examples of financial abuse that were raised with us include:
- perpetrators making a victim survivor a company director without their knowledge
- perpetrators selling a victim survivor’s property and keeping the money
- perpetrators withdrawing or forcing a victim survivor to withdraw large sums of money
- perpetrators accruing debts and fines in the victim survivor’s name.
Financial counselling can be an essential service to disrupt and stop the suffocating financial pressure and abuse a victim survivor may be experiencing, and to support recovery.
“Referrals to financial counsellors or living skills workers would be amazing for people who have escaped but are trying to get their life in order."
Kelly, victim survivor
The Department of Justice and Community Safety advised us that through the Financial Counselling Program, Consumer Affairs Victoria funds the equivalent of 21 full-time family violence financial counsellors across the state, which are located locally in a range of community services. These are in addition to the more than 300 generalist financial counsellors located across the state, who also work with clients impacted by family violence. The family violence financial counsellors provide specialist support to victim survivors to address financial abuse, improve the financial wellbeing of victim survivors, and provide expert advice to family violence services to improve financial outcomes for more victim survivors. Victim survivors can connect with the program through the National Debt Helpline, or they can be referred directly from other services. An example of how financial counselling can assist is demonstrated in Box 5.
Box 5: Case example demonstrating the importance of financial counselling
Around the time of the Royal Commission into Family Violence, Sally’s partner burnt her house to the ground. She was physically unharmed but was left homeless with her two children. Sally was connected with a financial counsellor through the local family violence service where the financial counsellor was co-located. The financial counsellor worked with a trauma-informed and client-centred approach with Sally’s housing worker, case worker and counsellor advocate to fully understand her situation and needs.
In order to allow Sally to focus on her immediate housing and court needs, the financial counsellor advocated to put Sally’s debt issues on hold to allow time for Sally to work through her immediate priorities (housing, court, counselling). After providing Sally with options in relation to her debts, she was successful in having the debts waived. Once Sally’s debts had been addressed and her insurance issues resolved, she decided her goal was to have her home rebuilt.
Insurance companies did not have a good understanding of family violence at that time. Sally’s insurance company interviewed her for more than three hours and she was made to feel like she was the one who burnt down the house. The financial counsellor worked closely with community legal services to advocate for changes to this approach and to support Sally’s claim, which was eventually settled. Through continued advocacy by many community groups, there have been changes and reforms in the insurance industry since that time.
The financial counsellor advocated for pro bono legal services for Sally, allowing for property orders to be completed while the perpetrator was in prison to ensure he could never receive financial benefit from proceeds that Sally would receive. The financial counsellor also advocated to the bank to waive more than $120,000 of debt, enabling her to afford to rebuild her family home.
Sally was able to move back into her house within two years.
Source: Based on a case described by Financial Counselling Victoria.
There are some key challenges and areas of improvement, though. For example:
- Financial Counselling Victoria explained to us that financial counselling is not currently an integrated part of the family violence service model [relates to action 5]. There is not a strong understanding of what financial counsellors can offer – for example, among staff at The Orange Door and specialist family violence services – except where there are existing relationships. Given the importance of financial security in supporting victim survivor recovery, we suggest further consideration should be given to how to embed this service within the model. We encourage active engagement and collaboration between Family Safety Victoria, Safe and Equal and Financial Counselling Victoria in working to embed financial counselling into the family violence response model.
- Consumer Affairs Victoria advised that the complexity of family violence cases means that many cases are taking longer, which reduces the number of clients a service can see and puts pressure on workers to take on more cases than they can manage [relates to action 13]. With only 21 full-time equivalent family violence financial counsellors statewide (10 of whom have no guaranteed funding after June 2023), this is a very limited resource. Furthermore, Financial Counselling Victoria spoke of capacity challenges for the 300+ generalist financial counsellors in Victoria, who face increasingly unmanageable caseloads. They suggest that to address this in the long term, funding models for family violence services need to incorporate provision for financial counselling as a matter of course. In the short term, funding certainty for the existing group of family violence financial counsellors is required, and adding more positions would help to alleviate the growing demand pressure.
The financial counselling sector also plays an important systemic advocacy role – for example, by advocating as a profession to banks, debt collectors and creditors around family violence policies and practices, and sharing experiences with the Economic Abuse Reference Group. This reference group, which is an informal, national network of nearly 30 community organisations (such as family violence services, community legal services and financial counselling services), works to influence government and industry responses to reduce the financial impact of family violence. Some key changes the group has influenced are captured in Figure 14.
Figure 14: Industry changes influenced by the Economic Abuse Reference Group

{kind=link}
For victim survivors who have suffered injuries through a violent crime, there is a process for accessing financial assistance to meet the costs associated with those injuries through the Victims of Crime Assistance Tribunal (VOCAT). Each year around a third of applications to VOCAT relate to family violence. Following the Royal Commission and a subsequent review by the Victorian Law Reform Commission, the government is replacing VOCAT with a new Victims of Crime Financial Assistance Scheme, which is expected to commence in late 2023. The new scheme will have a simpler and more victim friendly process, longer timeframes within which victim survivors of family or sexual violence can make an application (up to 10 years), and will be complemented by a new Victims Legal Service to assist people making applications under the scheme.
Legal and court supports
The court system is a common part of the victim survivor journey, with many victim survivors going through the process of securing family violence intervention orders (FVIOs) through the Magistrates’ Court of Victoria. Acknowledging that the intersection with courts can be very brief, there are some initiatives within courts that aim to improve the experience for victim survivors (see Figure 15). These are in addition to support available through police court liaison officers and community legal centres or duty lawyer services.
Figure 15: Key initiatives to support the experience of victim survivors at court
{kind=link}
These are widely seen to be important initiatives to improve the victim survivor experience in court and beyond; however, there are some challenges and areas for improvement. For example:
- In 2020–21 only a small proportion of finalised FVIO applications were heard in a specialist family violence court, meaning most victim survivors were not receiving a specialist response. With 12 specialist family violence courts now operational, and more to come, we have been advised that a growing majority of family violence matters will be heard in specialists courts.
- Pre-court engagement is an important way of connecting victim survivors with appropriate supports in the lead-up to their court appearance, but the full pre-court engagement model is currently only available in seven courts, and the program is only funded until 30 June 2023. An online portal has been created to allow The Orange Door and Victoria Police to directly provide to the court information relevant to the victim survivor’s needs, and this allows all specialist family violence courts to gain some advantage from pre-court engagement. However, the proactive engagement feature of the full model is a vital element, and we suggest that to realise the benefits of the model for both victim survivors and the court system, there would be value in ensuring pre-court engagement becomes an integrated and funded component of the specialist family violence court model.
- Victoria Legal Aid has provided strong feedback that the distinct needs of child victim survivors are not appropriately met in the court system, stating that children are not recognised independently of adult victims and do not participate in Magistrates’ Court FVIO hearings. Indeed, the Family Violence Protection Act 2008 mitigates against children’s voices being heard, stating that, for example, ‘a child, other than a child who is an applicant for a family violence intervention order or a respondent, must not give evidence for the purposes of a proceeding under this Act or a litigation restraint order proceeding unless the court grants leave for the child to do so’. While we understand the desire to protect children from harm associated with participating in the court system, we suggest further consideration must be given to ensuring the needs and wishes of children are independently assessed and considered [relates to action 3].
“As a child … I felt really excluded from court proceedings … Therefore a recommendation would be to check with what the child knows and what they want during key moments throughout the process. They may not want to know/care and that’s fine too – but providing some sense of autonomy and control would have been great."
Heshani, victim survivor
- The capacity of practitioners, duty lawyers and police liaison officers to attend court was also raised as a substantial challenge. These professionals have multiple cases to attend to every day and must therefore prioritise high-risk cases when managing their time. Duty lawyers will not have time to make referrals to relevant services for all clients and may instead provide pamphlets to clients who are deemed to be at lower risk. Similarly, family violence practitioners do not have the capacity to see every victim survivor who wants to see them on any given day. Furthermore, these practitioners are not available in every court, and concerns were raised with us about insufficient support for child victim survivors in all courts (children only have access to a child-specific family violence practitioner if they attend the Melbourne Children’s Court) [relates to action 3].
- Victoria Police expressed concern about victim survivors being encouraged by private legal practitioners, usually in cases where police are not involved, to agree to an Undertaking (‘a formal written promise’ from the respondent to the applicant). There was particular concern about some Undertakings including conditions that are counterintuitive, such as allowing the perpetrator to attend the victim survivor’s property for certain reasons. An Undertaking results in the FVIO application being withdrawn and is not enforceable by police.
- Further, while it is positive that victim survivors have more choice in how they engage with the court process, Victoria Legal Aid raised a concern that if victim survivors are not present in court, their opportunity to engage with a duty lawyer is reduced. This is problematic because the duty lawyer can help ensure the terms of the FVIO are workable for the victim survivor and refer them for broader legal support, including for any child protection or family law matters. However, where pre-court engagement is occurring, there is an ability to refer people to legal support before their court date, which means they don’t need to be in court to be connected with legal representation.
Victoria Legal Aid and the range of community legal services we met with were clear about the importance of victim survivors receiving early legal advice and expressed some frustration that legal support is not yet an integrated part of the family violence service system. Referrals can be made to legal services – for example, from The Orange Door or a specialist family violence service – but we understand that local arrangements for, and use of, such referrals vary. They also told us of substantial unmet demand, but they were constrained in their ability to address this due to their limited capacity and level of funding [relates to action 5].
“Being fairly and adequately represented is hard and we’re talking about access to justice to ensure you and your children are safe. It’s not a ‘nice to have’."
Jasmine, victim survivor
The structure of funding for duty services and other streams of legal assistance was also raised as a barrier for achieving continuity of legal support (or any legal support) across all client matters, which, as well as family violence matters, may include related legal areas such as family law, child protection, migration, criminal law and tenancy matters [relates to action 12]. The legal assistance sector is, therefore, forced to provide a very short term service, and victim survivors are then ‘bounced around the system as there is no capacity to get ongoing legal assistance’, as one stakeholder told us. Additionally, the Federation of Community Legal Centres and Victoria Legal Aid noted that legal services have not been provided any additional funding to support the newest seven specialist family violence courts (established in October 2022). This will limit their ability to implement the specialist family violence court legal practice model developed by Victoria Legal Aid in consultation with lived experience groups and other stakeholders.
The Department of Justice and Community Safety and Family Safety Victoria have recently begun a pilot that connects clients of The Orange Door network with legal services that meet their needs and ensures clients of legal services are effectively connected to The Orange Door for family violence and child wellbeing support. The pilot will run for 12 months and is being delivered at an Orange Door location. The pilot is guided by a service design model developed in close consultation with people with lived experience, The Orange Door network representatives and a broad range of legal services. This is an important project, and we suggest it will need to be closely monitored and evaluated to inform the broader inclusion of legal support within The Orange Door model [relates to action 12].
Therapeutic services
Therapeutic services for victim survivors have an explicit focus on supporting victim survivors to recover from the trauma of family violence.
The outcome of therapeutic interventions is to assist long-term recovery and wellbeing by rebuilding confidence, self-esteem and reducing social isolation.
Such interventions are supported through two funding streams:
- Family violence counselling for women and children, which has been a funded part of the family violence response for many years. Thirty per cent of funds must be allocated to services for children and young people.
- Family violence therapeutic interventions, which have been offered since 2019 by selected service providers in each of the 17 Department of Families, Fairness and Housing areas, building on lessons learnt from the 26 therapeutic intervention demonstration projects. We understand these interventions are now an ongoing feature of the system and can take a range of forms such as one-on-one counselling, coaching, family work, group work and ongoing peer support. The format depends on client and local needs and provider expertise. Forty per cent of funds must be allocated to services for children and young people.
Given the close relationship between the two streams, Family Safety Victoria has identified an opportunity to streamline the funding and to create an overarching framework for therapeutic services for victim survivors in Victoria. It would seem timely to generate such a framework, given that the latest guidelines for family violence counselling are from 2008, and that the only overarching information about therapeutic interventions is the 2019 call for funding submissions for the ongoing delivery of therapeutic family violence services to victim survivors.
Our fourth report to parliament noted that funding for therapeutic services for family violence victim survivors in 2019–20 ($32 million) represented a 366 per cent increase on the pre-Royal Commission level of investment ($7 million in 2014-15).70 We also note investments in recent years to expand services for adolescents who use violence at home, many of whom are also victim survivors.
Nevertheless, services are not meeting demand [relates to action 13]. While we have not seen any system-wide data, stakeholders consistently raised the issue of very long waitlists for therapeutic services, with some areas experiencing delays of six to 10 months for family violence counselling [relates to action 14]. One service provider said that over the course of these extended waiting periods, clients’ situations can dramatically change, sometimes declining to a point where, for example, a mother has lost housing and children have been removed from her care. Another service provider said they manage waitlists by restricting the number of family violence referrals they accept, and instead refer them back to The Orange Door or a specialist family violence service because it is too risky to have them sitting on a waitlist with no support. The wait time at this service was said to be four weeks.
For some groups, there are further delays and access barriers. For example, refugee and migrant women may need a counsellor who speaks a language other than English, which can be difficult to find. Thorne Harbour Health indicated that GBTQ male victim survivors who are referred to a Centre Against Sexual Assault have reflected a sense of being misunderstood and seen as too complex by sexual assault services. They have observed a lack of literacy around intimate partner sexual violence within the LGBTIQ+ community. We note that the need to improve the inclusiveness of services and to increase capability around diverse experiences of abuse are common themes across the family violence and sexual assault sectors. Sexual Assault Services Victoria explained that it, along with its members, continues to work to improve inclusive, culturally safe practices in delivering sexual assault services. For example, it now employs dedicated LGBTIQ+ and disability-focused inclusion officers to help strengthen inclusive practice across the specialist sexual assault sector.
Many stakeholders, ranging from victim survivors to legal services and peak bodies, despaired at the lack of targeted and easily accessible therapeutic services for children. The Centre for Excellence in Child and Family Welfare told us that even mothers who have the means to pay for private support for their children do not know where to go for help. Some stakeholders also raised questions about whether the therapeutic interventions that were being provided to children were sufficiently targeted at children’s unique needs, with a common belief that ‘if Mum is ok, the kids are ok’. We are not aware of any monitoring of the services provided using the counselling and therapeutic interventions funding but suggest this may be an area for further investigation [relates to action 14]. The Royal Commission was clear about the need for child victim survivors to have access to such support and noted ‘if we do not provide this support, the effects of family violence suffered by children may be carried on to the next generation’.
In some cases, because of the known delays in accessing the free therapeutic supports designed for victim survivors, Flexible Support Packages are being used to access private psychologists. This may or may not at times be suitable, but stakeholders told us that this practice may not represent an efficient use of response system funding, particularly because the private system is more expensive, suggesting instead that the supply of funded therapeutic services needs to increase [relates to action 13].
Footnote
- Note: This is based on the 2019–20 figure for social housing allocations (5,414) and the December and March 2021 number of applications on the Victorian Housing Register. We have not seen more recent figures for the number of social housing allocations but suggest the number may be even lower, given the statement in the Department of Families, Fairness and Housing’s most recent annual report that there has been a ‘decrease in tenants moving out of public housing which has provided fewer opportunities to allocate properties to people on the register’. See Department of Families, Fairness and Housing (2022): Annual Report 2021–22, p. 50.
Recovery and healing
Longer term support and a more holistic approach are required to support recovery and healing
The Royal Commission identified three pillars of recovery – secure and affordable housing, financial security, and health and wellbeing – and highlighted the need for adequate support in each of these areas to help victim survivors rebuild their lives. Support available in these pillars has been covered throughout this report, but as has already been raised, there are substantial issues in the capacity of these services to meet demand and provide support in a coordinated way to meet an individual’s needs. Support is also often time-limited, which many stakeholders told us does not reflect the needs of victim survivors over time. There is a need for longer term models of support to allow victim survivors to heal, which likely needs to
include a defined role for the health and mental health systems, and peer support.
Importance of long-term support
The National Plan to End Violence Against Women and Children 2022–2032 recognises that ‘recovery and healing takes time and victim-survivors will, in many cases, require life-long support through dedicated and tailored services and interventions’. Yet one of the pieces of feedback we most consistently received during our consultations was that a clear crisis to recovery model has not been articulated. Powerfully, the CEO of Safe and Equal told us that:
The system has never been funded for recovery. We know that recovery is a long journey, and it is not linear or predictable. We need to continue to build the evidence base for what supports long term recovery, but at the very least, we need investment in the system for ongoing therapeutic supports so that victim survivors can access a range of options based on their individual needs, when they need it.
Similarly, Djirra said:
There is no talk about what [recovery and support] looks like over the lifetime … no ongoing holistic recovery from trauma, especially intergenerational trauma; it doesn’t exist at all.
This affects the ability of services to provide the long term support that victim survivors need. Djirra noted that this is particularly relevant to Aboriginal services:
Aboriginal services are working with women who have complex and often multigenerational trauma and require long term and specialised support for themselves and their families.
The system is said to be geared towards crisis and the period immediately afterwards. While this is somewhat understandable in the context of overwhelming demand, it means there is likely an insufficient focus on recovering from the trauma of family violence, and victim survivors often feel prematurely disconnected from support. Ironically, cutting support short for victim survivors because of demand pressure may result in victim survivors returning to the perpetrator, ending up in similar relationships in the future and/or continuing to struggle with the ongoing negative impacts of family violence, thereby increasing the level of support they are likely to need in the future. For some victim survivors, the family violence may continue for many years, even after separation, such as in cases where there is shared custody of children.
We heard a number of examples that illustrate the types of longer term support that might be effective:
- One victim survivor was extremely grateful for a sexual assault service worker who she said helped give her a sense of hope and empowerment. With the support of the worker, the victim survivor was able to consider her own strengths, skills and knowledge and use this to get a job and regain control of her life.
- Another victim survivor experienced depression and anxiety during pregnancy and had the support of PANDA (Perinatal Anxiety & Depression Australia). The service called her weekly throughout the pregnancy, just to check in, and the victim survivor said she found this extremely supportive and an important way to be connected with other services when she was not okay. She wonders if a similar model could be applied to family violence.
- The sexual assault service sector was said to be better at recognising the need for victim survivors to be able to reconnect with a service over time as life events trigger past trauma. For example, the Goulburn Valley Centre Against Sexual Assault explained that it is funded to deliver support across a person’s lifetime, and that it is very common for victim survivors to transition in and out of the service over many years depending on their needs. Stakeholders noted that the family violence system does not work in this way, although the call for funding submissions to deliver therapeutic family violence services does indicate a similar model:
Recovery from family violence can take a long time for some victim survivors whose support needs may fluctuate and change through the sustained healing process. Everyday life events have the potential to negatively trigger a victim survivor who may require re-engagement with services. It is important that clients know that when they leave the service that they are still supported by the provider and can seek further assistance in the future, whether through a service offered by that provider or through referral to another one (in the broader sector) that can best fit their needs.
- McAuley Community Services for Women spoke about the value of the simple act of periodically hosting lunches where any client, past or present, can attend, reconnect with the service and chat with other victim survivors.
Ongoing role of the health sector
The call for funding submissions to deliver therapeutic interventions included a section on ‘transition to community support and sustained support’, stating that ‘the purpose of the transition process is to ensure clients have sustained and ongoing support as they continue on their recovery process’. Successful providers were required to either plan to support clients’ ongoing therapeutic recovery after an intervention or ‘demonstrate the process for transitioning clients to sustainable recovery pathways’. One likely source of ongoing support is the broader health and mental health sector [relates to action 7].
According to the 2017 Victorian Population Health Survey, 66.7 per cent of women and 36.4 per cent of men who experienced family violence had been diagnosed by a doctor with depression or anxiety (see Figure 16), compared with 31.3 per cent of women and 20.7 per cent of men who did not experience family violence. However, victim survivors have expressed that the mental health system is not working for people from low-socioeconomic communities or with complex trauma, with access to free services subject to excessively long waitlists.
Figure 16: Victim survivors diagnosed with depression or anxiety
Source: 2017 Victorian Population Health Survey
The Royal Commission into Victoria’s Mental Health System (RCVMHS), which handed down its final report in March 2021, acknowledged family violence as a driver of mental ill health and provided a blueprint for a redesigned mental health system. We have seen little evidence of coordination between the mental health and family violence reforms, but we anticipate the implementation of several of the RCVMHS’s recommendations will improve the quality of and access to mental health services for family violence victim survivors. For example, the RCVMHS recommended a new approach to addressing trauma in Victoria, supported by a new statewide trauma service. This new approach will also include the placement of specialist trauma practitioners in each of 22 new Adult and Older Adult Area Mental Health and Wellbeing Services, along with the 13 new Infant, Child and Youth Area Mental Health and Wellbeing Services. We suggest ongoing coordination of the implementation of both sets of reforms will be essential, and many family violence sector stakeholders have called for the clear articulation of the mental health system’s role in victim survivor recovery.
“Children from families experiencing family violence should be overseen by a consistent and appropriately trained child psychologist, for the duration of their childhood."
Lily, victim survivor
As we raised in our Early Identification of Family Violence Within Universal Services report, patients often have close, trusting and extended relationships with their general practitioner, so it makes sense to use this connection for ongoing monitoring of a victim survivor’s wellbeing. However, as the Royal Australian College of General Practitioners has raised with us, the available Medicare items do not cover family violence, long consultations are not financially supported, and while victim survivors often present with both physical and mental health issues, Medicare does not allow GPs to bill for both mental and physical health on the same day.
The Royal Commission raised the need for Medicare reform, recommending:
The Victorian Government, through the Council of Australian Governments, encourage the Commonwealth Government to consider a Medicare item number for family violence counselling and therapeutic services distinct from a general practitioner mental health treatment plan. In the longer term consideration should be given to establishing a Medicare item number or a similar mechanism that will allow medical practitioners to record a family violence–related consultation or procedure and so more accurately ascertain the public cost of family violence. (Recommendation 105)
We suggested similar action in our Early Identification of Family Violence Within Universal Services report. We note that the creation of any new family violence–related Medicare item(s) would need to be accompanied by safety measures to ensure perpetrators on the same Medicare card would not be able to look up the card’s claims history and see that a family violence consultation had occurred.
Unfortunately, the National Plan to End Family Violence Against Women and Children does not mention the need for changes to Medicare to better allow GPs and others to support victim survivors, although it does acknowledge Medicare as an Australian Government system with a role to play in ending family violence. We suggest there is still an opportunity to highlight action in this area through the two action plans that will be developed to implement the national plan [relates to action 4].
“We need long-term access to mental health supports for victim survivors and their children and the opportunity for stability through stable housing, access to a stable income. Until we have stable basic needs – like safety, food and shelter – how can we recover?"
Jasmine, victim survivor
Peer support
Building on the discussion in other sections of this report about the potential role of a more structured lived experience workforce in the family violence sector, many victim survivors we consulted with told us of the healing power of connecting with their peers through lived experience groups like the Victim Survivors’ Advisory Council. It was an important part of their journey towards recovery. Sector stakeholders similarly spoke of the power of bringing victim survivors together for the purpose of building their peer connections and supporting their recovery, and they shared examples of effective peer support programs (see Box 6 for an example). However, these programs were locally driven and not centrally funded, which means victim survivor access to such programs is variable. The programs are also not always well-known and understood by other parts of the service system, even locally, which made it difficult to get referrals.
“Peer support is such a great support service. It facilitates both a connection back into the community but also the ability to reflect and express experiences in a safe place." - Heshani, victim survivor
“It helps to have people who can relate to you and know what you’ve been through." - Jasmine, victim survivor
There are also examples of child- and youth-focused group programs that contain a peer support element (see Box 7 for one example). As a Berry Street Y-Change Lived Experience Consultant powerfully stated:
Family violence is rarely seen or understood through the eyes of children and young people. Way too often, we are the ones you leave behind.
It would be worth considering whether and how such programs could be made available to support more children and young people who have experienced family violence to ensure they feel seen and heard [relates to action 6]. More broadly, we suggest there is likely great value in establishing peer support as a more consistent part of a suite of supports available to victim survivors as part of their recovery. One suggestion worthy of consideration was to have peer support groups running alongside all specialist family violence services.
“Often people have lived with a great deal of violence and control and doing basic things like washing, cleaning, cooking, and paying bills or general routine for everyday life is a struggle. I think starting from the beginning and working through general life would be helpful, it could even be a support group type environment, maybe even run by peer groups..."
Kelly, victim survivor
Box 6: The DAWN mentoring program
The Doncare Angels for Women Network (DAWN) mentoring program is a long-term support program for women who are recovering from the impacts of family violence. Trained volunteer mentors are matched to the women based on mutual interests, location and availability. The program aims to improve safety and build confidence and community connectedness among victim survivors. Mentors provide weekly support by assisting with access to services like financial counselling, women’s support groups, and court and legal services. They act as a source of companionship at a time when many victim survivors can feel isolated. This support spans 12–24 months. It has been estimated that over half of the volunteer mentors have had experience themselves of family violence, either directly or through friends or family members, and can help women navigate the system and learn what services are available to them.
Clients are referred to the DAWN program by family support workers, counsellors, emergency relief workers, women’s refuges, other welfare services and police. The program began in 2007, with Australian Government and philanthropic funding for the first two years. It has largely been funded by Manningham City Council since 2009; however, more recently, funding from the Ian Potter Foundation has allowed it to expand beyond the Manningham catchment to include the cities of Whitehorse, Maroondah, Monash, Boroondara, Knox and Banyule.
A 2016 evaluation of the DAWN program assessed the program’s impacts since its development in 2007. This found significant reductions in levels of depression, anxiety and stress for surveyed clients post the DAWN program. The women also generally reported feeling calmer, happier, more hopeful and that they were managing better. It also noted the positive side effect of improvements in the quality of life for the children involved, once the mothers felt supported and more confident.
Source: Based on advice provided by the Eastern Metropolitan Regional Family Violence Partnership and Doncare (2016), Doncare Angels for Women Network Evaluation Report 2007–2016.
Box 7: Feeling Visible pilot program for young people
WRISC Family Violence Support offers wraparound services and programs for children and youth living in the Central Highlands region. It is piloting a six-week, school-based, small group program – Feeling Visible – run by a registered art therapist. The program caters for students demonstrating the impacts of family violence. Students are engaged using an art-based, trauma-informed approach.
The program uses a peer support model to foster connections with others in the group who have had similar experiences. It enables them to build confidence and connections with others in a shared space to develop a personal language to describe their experiences.
The evaluation of the pilot at one school showed that the vast majority of participants felt a strong sense of safety while participating in the group sessions, with one student commenting that their ‘favourite part was going around the circle and talking about it together’.
The facilitator of one of the pilot programs reported that participants, through peer support, are developing and learning ways to understand their experiences and what they need in order to heal, enabling them to make healthy choices when feeling overwhelmed and notice what their bodies are telling them about their physical and emotional safety.
One of the benefits identified through the evaluation came from one of the pilot school’s mental health practitioners:
I have observed the students being more connected to each other and to wellbeing, breaking down some of the stigma around family violence and help seeking in general, they have felt seen and validated in their experiences [and] they have had a positive experience of a therapeutic relationship, having a chance to have ‘voice and choice’, and they have learned gently and in a non-threatening way about family violence.
Source: Based on information provided by WRISC Family Violence Support, including a program evaluation.
Other issues
Child FIRST
While technically out of scope for this report, several stakeholders raised concerns about a perceived shift in focus of Child FIRST since it became part of The Orange Door. Child FIRST (child and family information, referral and support teams) is the entry point into services that support families who need assistance with the care and wellbeing of children.
Anglicare Victoria explained that while The Orange Door is also meant to be the gateway into child, youth and family services, it is commonly viewed as primarily a family violence service, and they often see less attention on outcomes for families needing support unrelated to family violence. They explained that, like the family violence system, the child, youth and families system in some areas is overwhelmed with demand, meaning that families only enter the service system when their situation has deteriorated, when this could have been prevented from happening with earlier intervention. Similarly, the Centre for Excellence in Child and Family Welfare explained that Child FIRST previously had a greater focus on providing early parenting help to ensure children could thrive, but that now this function has weakened. It stated that there is an urgent need to carve out the early intervention role of Child FIRST once again. The Department of Families, Fairness and Housing has advised that work is underway to develop a child wellbeing assessment tool that will be used in The Orange Door to ensure a child wellbeing focus is maintained.
We were also told of stigma associated with using a service commonly considered to be family violence– focused, and this may be a barrier to engagement for some families.
Glossary
| Aboriginal | While acknowledging the diversity of Aboriginal people in Australia, in this document the term ‘Aboriginal’ has been used to refer to all people of Aboriginal and/or Torres Strait Islander descent. |
| Affected family member | A person who has experienced family violence, also known as a victim survivor. The term is predominantly used in police and court proceedings to refer to the person to be protected by a family violence intervention order. |
| Applicant | A person who applies for a family violence intervention order. This can be a Victoria Police member applying on behalf of the affected family member. |
| Case management | A collaborative support service for both victim survivors and perpetrators of family violence. Case managers assess risk, develop safety plans and goals, monitor progress and provide a connection to a range of required services, based on individual needs. |
| Child FIRST | Child and Family Information Referral and Support Teams (Child FIRST) aims to link vulnerable children, young people and their families to the support they need. It is a central referral point to a range of community-based child and family services within local catchment areas, and is now located within The Orange Door model. |
| Child Protection | Child Protection receives and investigates reports of child abuse, risk of significant harm to children or children being inadequately cared for by their families. It can refer children and families to support services and, where required, can make applications for protection orders to the Children’s Court for the protection and permanent care of children. It is also responsible for administering protection orders made by the court. |
| Community services | Local support services for individuals and/or families that may include information, advice, practical help, financial help or a combination of services. Community services often address the needs of diverse groups. |
| Diverse groups | Groups that may have different experiences of family violence and different needs, and who may be experiencing additional barriers to seeking help and receiving support due to particular background or personal characteristics. These include children and young people, older people, Aboriginal and Torres Strait Islander peoples, people within culturally and linguistically diverse communities, people within the LGBTIQ+ community, people living in rural, regional and remote communities, people with a disability, male victims, women prisoners and women who work in the sex industry. |
| Family Safety Victoria | A division of the Department of Families, Fairness and Housing (comprising some portfolio responsibilities of the former Department of Health and Human Services) with dedicated responsibility for delivering key elements of family violence reform. This includes the Family Violence Information Sharing Scheme, The Orange Door network and the Family Violence Multi-Agency Risk Assessment and Management reforms. |
| Family violence | Any violent, threatening, coercive or controlling behaviour that occurs in current or past familial relationships, including by intimate partners, family members and/or nonfamily carers. |
| Family Violence Information Sharing Scheme |
Established in legislation, the scheme enables sharing of information between authorised organisations to support the assessment and management of family violence risk. |
| Family violence intervention order (FVIO) |
A court-issued order to protect people from further family violence. |
| Family Violence Multi- Agency Risk Assessment and Management (MARAM) Framework |
A framework to help identify, assess and manage family violence risk. A range of organisations are required by law, under the Family Violence Protection Act 2008, to align their practices and policies with MARAM, which replaced the former common risk assessment framework or ‘CRAF’. The MARAM Framework is supported by operational practice guidance and risk identification, screening and assessment tools. |
| Family Violence Report | Risk assessment and management tool completed by Victorian police officers after every family violence incident. Reports are informed by the officer’s observations and include an assessment of the severity of risk based on responses from all parties involved. Reports automate referrals to The Orange Door, community agencies and/or Child Protection, where required. Also known as an ‘L17’. |
| Family Violence Safety Notice | A police-issued notice that provides immediate protection for a victim survivor by placing temporary conditions on a family member who is using family violence before an intervention order application is heard in court. |
| Intersectionality | Describes how systems and structures interact on multiple levels to oppress, create barriers and overlapping forms of discrimination, stigma and power imbalances based on characteristics such as Aboriginality, gender, sex, sexual orientation, gender identity, ethnicity, colour, nationality, refugee or asylum seeker background, migration or visa status, language, religion, ability, age, mental health, socioeconomic status, housing status, geographic location, medical record or criminal record. This compounds the risk of experiencing family violence and creates additional barriers for a person to access the help they need.+ |
| LGBTIQ+ | An inclusive initialism that refers to lesbian, gay, bisexual, transgender / gender diverse, intersex and queer people. |
| MARAM | See Family Violence Multi-Agency Risk Assessment and Management (MARAM) Framework. |
| Principal Strategic Advisor | A key leadership position in each of the Department of Families, Fairness and Housing areas. Principal Strategic Advisors lead local Family Violence Regional Integration Committees and have a strong focus on integration and collaboration of services, driving implementation of the reforms and capacity building of the workforce. |
| Respondent | A term used by police and the courts to describe the alleged family violence perpetrator. They are the person against whom an application for an intervention order has been made, or against whom an intervention order or Family Violence Safety Notice has been issued. |
| Response | Family violence 'response' refers to the model and specialist family violence service system designed to respond to cases of family violence by supporting victim survivors and holding perpetrators to account. It aims to prevent the re-occurrence of violence. |
| Royal Commission into Family Violence | Established in 2015, the Royal Commission was tasked with finding ways to prevent family violence, improve support for victim survivors and hold perpetrators to account. The Royal Commission provided its report, which included 227 recommendations, to the Victorian Government on 29 March 2016. |
| Safe Steps | A 24/7 statewide specialist support service for victims of family violence. Services include information and referral, crisis response, specialist family violence risk assessment, safety planning, and access to supported crisis accommodation. |
| Specialist Family Violence Court | Specialist court model delivered through the Magistrates' Court of Victoria that provides enhanced safety features including separate entrances for victim survivors and remote hearing facilities. Specialist Family Violence Courts are staffed by specially trained magistrates and court staff, partner agencies and other court-based services to deliver a coordinated response. Magistrates at Specialist Family Violence Courts have powers to mandate counselling orders for perpetrators. |
| Specialist family violence services | Services with expertise in family violence that provide crisis responses and case management to victim survivors. |
| Statewide Family Violence Integration Advisory Committee | A statewide group that supports discussion, collaboration and knowledge building across Family Violence Regional Integration Committees, and provides a linkage mechanism to connect local committees with Family Safety Victoria and other statewide bodies. Consists of Principal Strategic Advisors from across the state. |
| The Orange Door | A network of local entry points to women’s and children’s family violence services, services for men who use violence and family services. It undertakes triage to assess and manage risk and connect people to the services they need. |
| Therapeutic interventions | Facilitated by a professional practitioner, actions designed to improve an individual’s health and wellbeing as a result of family violence trauma. Intervention responses include group sessions, family work, individual counselling, coaching and ongoing peer support, with the long-term goal of rebuilding self-esteem and confidence and reducing social isolation. |
** Definition from Department of Premier and Cabinet (2017): Free From Violence: Victoria’s Strategy to Prevent Family Violence and all Forms of Violence Against Women.
+ Definition from Department of Premier and Cabinet (2018): Everybody Matters: Inclusion and Equity Statement.
Acknowledgement of Traditional Owners
The Victorian Government proudly acknowledges Victorian Aboriginal people as the First Peoples and Traditional Owners and custodians of the land and water on which we rely.
We acknowledge and respect that Aboriginal communities are steeped in traditions and customs built on an incredibly disciplined social and cultural order. This social and cultural order has sustained up to 60,000 years of existence.
We acknowledge that Aboriginal communities includes both Aboriginal and Torres Strait Islander people living in Victoria.
We acknowledge the ongoing leadership role of the Aboriginal community in addressing and preventing family violence and join with our First Peoples to eliminate family violence from all communities.
Recognition of victims and survivors of family violence
We acknowledge the terrible impact of family violence on individuals, families and communities, and the strength and resilience of the children and adults who have, and are still, experiencing family violence.
We pay respects to those who did not survive and to their family members and friends.
Family violence services and support
If you are concerned for your safety or that of someone else, please contact the police in your state or territory, or call Triple Zero (000) for emergency assistance.
If you have experienced family violence and need support or assistance, contact:
National Sexual Assault and Domestic Violence hotline 1800 RESPECT (1800 737 732)
Safe Steps 24/7 family violence response line 1800 015 188
Victims of Crime helpline for men who are victims of family violence 1800 819 817 (8am-11pm)
Rainbow Door specialist LGBTIQ+ support, advice and referral line 1800 729 367 (10am–5pm).
If you are concerned about your behaviour and its impact on your family, contact the Men’s Referral Service on 1300 766 491 (24/7 service).
Child and youth friendly report summary
This is a summary of the Crisis response to recovery model for victim survivors report which has been prepared in partnership with Berry Street’s Y-Change initiative.

Welcome to the report summary
Message from the Monitor
Throughout our monitoring we have been guided and challenged by young people who are victim survivors of family violence. The voices of these young advocates must be heard as they know best what is needed to keep them safe and to support their recovery. This report summary is the result of their knowledge and wise guidance. It has been prepared by young people in language that is clear and meaningful to them and their peers. We are indebted to these courageous champions of change who are committed to using their lived experience to shape the service system so that it can meet the needs of young people.
Jan Shuard PSM
Family Violence Reform Implementation Monitor
Message from Y-Change
Family violence is rarely seen or understood through the experiences of children and young people. Too often, we are the ones you leave behind. It is critical to recognise us as victim survivors in our own right, not as ‘secondary victims’ of family violence or ‘extensions’ of our mother. Working in partnership with children and young people must be placed centrally to system reform. We hope that one day, our visions for change directly inform research, policy and practice reforms, and broader social change in a way that becomes everyday practice. That people understand that reform is not just something that happens ‘in the system’, it begins with each of us – our mindsets, approaches, and capacity to be challenged by young people with lived experience.
Berry Street’s Y-Change initiative
Acknowledgements, content warning and support and a thank you
Acknowledging Aboriginal and Torres Strait Islander peoples, recognising people with lived and living experience and a thank you to the Berry Street Y-Change Lived Experience Consultants.
Acknowledgements
We proudly acknowledge the Australian Aboriginal and Torres Strait Islander peoples of this nation as the traditional custodians of the lands, waters and seas. We pay our respects to Elders past and present and honour the survival of Indigenous Australians. We recognise the continued impacts and violence of colonisation and our role in taking apart systems that cause harm.
We would like to recognise the lived and living experience of people who have or are still going through family violence, or who have lost their lives due to family violence.
We would like to thank the young Lived Experience Consultants from Berry Street’s Y-Change initiative for working with us to develop and write this child and youth-friendly summary.
Content warning and support
In this summary, we talk about some hard topics such as family violence, homelessness, grief and loss. Please go gently with yourself as you read through the report. If you need support, there are services you can reach out to. You can find their contact details towards the end of this summary.
Words that are bolded are explained in the definitions page.
What is the Crisis response to recovery model for victim survivors report about?
A brief description of the report and 16 suggested actions for government to consider.
In 2022 we spoke to victim survivors and professionals about the challenges navigating the service systems and their ideas for change. Where possible we have included the expertise of people with a lived experience in our reports.
We wanted to hear directly from victim survivors about their experiences getting help when facing family violence and from workers about how the system responds to victim survivors at their point of crisis.
We kept coming back to these key points which guided our conversations:
- how victim survivors felt when trying to get help or reach out
- if there were enough services to help victim survivors
- if services were meeting the needs of a diverse range of people
- whether there was enough focus on long-term recovery
- if services did offer help when victim survivors needed it.
Family violence can look like hitting, punching, screaming, threatening, speaking down to, controlling behaviours and getting people to do sexual things they don’t want to. It could also look like hearing, seeing or being around the impacts of violence. It may leave people feeling scared, unsafe, alone, and physically hurt. These are just some of the ways people can experience family violence.
How did we get here?
After a number of family violence deaths in Victoria, the Victorian State Government held a public investigation in 2015, called a Royal Commission(opens in a new window), to find ways to stop family violence from happening and improve the support available. The Royal Commission said that it was important to keep victim survivors safe, and to help people who are violent towards their family to change their behaviour.
It also said that all family violence services, and some public services (support services, police, courts) were overwhelmed, and could not keep up with the number of people asking for help. It found at the time that there was a lack of resources to help children and young people experiencing family violence. And that there was not enough support for victim survivors to help them recover from violence and rebuild their lives.
To follow up after the Royal Commission, the Government chose Ms Jan Shuard PSM as the second Family Violence Reform Implementation Monitor. Together with her team, they wrote the Crisis response to recovery model for victim survivors report that looks at the Victorian Government’s progress in helping victim survivors at their point(s) of crisis, and in their journey towards recovery.
The Monitor’s job was to find out what was happening in the family violence implementation space, and what things could be done better. This is now finished, and the final report has been given to the Premier of Victoria, the Minister for Prevention of Family Violence and other government leaders. The report provides 16 proposed actions for government to consider as it moves into the next stage of the family violence reforms (see next page for full list).
This is a summary of the Crisis response to recovery for victim survivors report which has been prepared by the Office of the Family Violence Reform Implementation Monitor (FVRIM) in partnership with Berry Street’s Y-Change initiative.
16 suggested actions for the Victorian Government to consider
The report provides 16 suggested actions for government to consider as it moves into the next stage of the family violence reforms.
Below are all the actions we suggested to the Victorian Government in our report that we think would help make the system better for victim survivors. The actions have been grouped together under related areas.
Taking a more victim-centred approach
- Be clear about whose job it is to help victim survivors work out what help they need.
- Find ways for workers from police, courts, The Orange Door and family violence services to work better together
- Act to make sure that children and young people are seen as victims in their own right and have a say in family violence–related court hearings.
- Keep asking the Australian Government to fix the problems that we know affect victim survivors in the following areas: immigration law, Medicare, Centrelink and the family law system.
Make sure victim survivors can access the supports they need
- Make sure that victim survivors can get help with financial support and the law.
- Make peer support workers available for victim survivors to help in their recovery.
- Make it clear about how the mental health system works with the family violence system to help support victim survivor recovery.
- Look at getting male victim survivors their own family violence help.
More support for the workers that help victim survivors
- Make sure that workers in family violence and sexual assault services have better pay and more secure work.
- Help services understand how to employ people, such as victim survivors, who might not have a university degree, but have the expertise.
- Look at how the mental health system has been able to give people with lived victim survivor experience the chance to work in the system to help other victim survivors.
Funding to help services support victim survivors' needs
- When giving funding to services, make sure they are focused on providing victim survivors with a good experience every time.
- Ask for more things that victim survivors need, like housing, help with paying rent and mortgages, help from lawyers about legal problems, financial support and other supports.
More data and monitoring to understand the issue
- Get better information about how many people are wanting help, and how long it is taking them to get that help.
- Look at how people move through the system to see what problems there are and fix them to make it easier to get help, including for children and young people.
- Keep looking at and understanding service data to fix problems and delays with The Orange Door.
1. More awareness, more delays
More people are aware of family violence and its impacts than ever before, but it can still be difficult to get help.

When the system response is that you’re on a waitlist for months, that’s so sad. Sleeping rough on the street can be worse than the abusive relationships. – Victim Survivors’ Advisory Council member
There is a lot of pressure on workers and organisations because of this increase in awareness, and they are not always able to help everyone the way they would like to.
For many people, the entry point into family violence services is through Victoria Police. Police members are given clear guidance on prioritising safety and support for children, young people and families, responding to the diverse needs of communities and looking at what is best for the child separate from parents and caregivers. But there are still barriers for people to report and access support this way.
Some of the other services where people going through family violence can get support are The Orange Door and the Safe Steps Family Violence Response Centre. Although these services provide support, we have heard victim survivors having to wait a long time before getting the help they need.
But what can be done?
We have suggested the following actions for the Victorian Government to tackle these problems (see full list for all 16 suggested actions(opens in a new window)):
Taking a more victim-centred approach
- Be clear about whose job it is to help victim survivors work out what help they need.
- Find ways for workers from police, courts, The Orange Door and family violence services to work better together
Make sure victim survivors can access the supports they need
- Look at getting male victim survivors their own family violence help.
More data and monitoring to understand the issue
- Get better information about how many people are wanting help, and how long it is taking them to get that help.
- Look at how people move through the system to see what problems there are and fix them to make it easier to get help, including for children and young people.
- Keep looking at and understanding service data to fix problems and delays with The Orange Door.
2. Traffic jam, moving slowly ahead
Family violence workers and services are so busy they are not always able to help victim survivors when they need it.
"When a survivor is forced to share parenting with a perpetrator, it is near impossible to recover. Perpetrators do not co-parent, they counter-parent. Survivors need ongoing, long-term supports in navigating endless coercively controlling behaviour." – Lily, victim survivor
Family violence workers and services are so busy they are not always able to help victim survivors when they need it. Once a victim survivor has accessed The Orange Door or Safe Steps, they can be referred to get case management support from a family violence service. After sitting on long waitlists, they may only get support from family violence workers for up to three months. But workers have said that this is not long enough, and that support is ending before victim survivors are ready. This leaves people to find more help and navigate the complex service system alone.
Services have been given more money to help people over the past few years, which has included the creation of The Orange Door as the main entry point for victim survivors to share their experiences and access the supports they need. But some victim survivors are having to retell their experiences many times to different workers and by the time the workers can help, they may not need that type of support anymore. There needs to be more thought into developing the service system beyond this point to ensure there are more support options available.
But what can be done?
We have suggested the following actions for the Victorian Government to tackle these problems (see full list for all 16 suggested actions(opens in a new window)):
Taking a more victim-centred approach
- Be clear about whose job it is to help victim survivors work out what help they need.
Make sure victim survivors can access the supports they need
-
Look at getting male victim survivors their own family violence help.
Funding to help services support victim survivors' needs
-
Ask for more things that victim survivors need, like housing, help with paying rent and mortgages, help from lawyers about legal problems, financial support and other supports.
More data and monitoring to understand the issue
-
Get better information about how many people are wanting help, and how long it is taking them to get that help.
- Look at how people move through the system to see what problems there are and fix them to make it easier to get help, including for children and young people.
3. Too many tasks, not enough tentacles
Family violence workers are leaving their jobs for lots of different reasons, such as the ongoing impacts of COVID-19, burnout, insecure work (short contracts) and low pay.

“Pre-COVID, many community service organisations struggled to secure enough new workers to fill vacancies. Workforce shortages were particularly acute in regional areas. These workforce pressures have been exacerbated by COVID-19, with exponential growth in demand for social assistance…The prolonged nature of the pandemic has left staff stressed and exhausted”. – Victorian Council of Social Services
Family violence workers are leaving their jobs for lots of different reasons, such as the ongoing impacts of COVID-19, burnout, insecure work (short contracts) and low pay. This is having a big impact on victim survivors getting help because there are not as many workers to support people.
The family violence workforce plays a very important role in the recovery of victim survivors and must be supported to do so. Workers and organisations told us that government can support staff wellbeing by paying workers more in the community sector and making sure they have stable jobs.
Victim survivors told us how rewarding it is to support and/or advocate with other victim survivors by engaging in lived experience work. But it is not always easy to know how to find these opportunities and how to make this type of work a career. There is an opportunity to have more lived experience workers in the family violence sector to provide peer support to many victim survivors recovering from family violence.
But what can be done?
We have suggested the following actions for the Victorian Government to tackle these problems (see full list for all 16 suggested actions(opens in a new window)):
More support for the workers that help victim survivors
-
Make sure that workers in family violence and sexual assault services have better pay and more secure work.
- Help services understand how to employ people, such as victim survivors, who might not have a university degree, but have the expertise.
- Look at how the mental health system has been able to give people with lived victim survivor experience the chance to work in the system to help other victim survivors.
4. Together we can do so much
The ways to get help can be very confusing for victim survivors, especially when they need support from lots of different places.
As a child … I felt really excluded from court proceedings … therefore, a recommendation would be to check with what the child knows and what they want during key moments throughout the process. They may not want to know/care and that’s fine too – but providing some sense of autonomy and control would have been great. – Heshani, victim survivor
The ways to get help can be very confusing for victim survivors, especially when they need support from lots of different places. Housing, school, work, health and wellbeing, court and the legal system are just some of the areas people may need support from. This can end up being left to the victim survivor to talk to all the different people involved, or they can get completely left out of conversations about their own life.
There are some good examples of coordination in local areas where workers are supporting victim survivors in a wraparound way to get the support they need. Unfortunately, this is not being supported by the broader systems because of a lack of money and strict reporting needs. It is important that family violence workers who help with lots of different supports keep talking and working with each other, so individuals and families get the help they need without having to retell their experiences over and over again.
The Royal Commission spoke about the need for a service navigator role which would work with victim survivors to provide practical, guiding, timely support from crisis through to recovery. There needs to be more clarity about whose role it is to do this. There may be an opportunity here for lived experience workers to provide this support to victim survivors.
But what can be done?
We have suggested the following actions for the Victorian Government to tackle these problems (see full list for all 16 suggested actions(opens in a new window)):
We have suggested actions 1, 2, 4, 5 & 12 for the Victorian Government to tackle these problems.
Taking a more victim-centred approach
- Be clear about whose job it is to help victim survivors work out what help they need.
- Find ways for workers from police, courts, The Orange Door and family violence services to work better together
- Keep asking the Australian Government to fix the problems that we know affect victim survivors in the following areas: immigration law, Medicare, Centrelink and the family law system.
Make sure victim survivors can access the supports they need
-
Make sure that victim survivors can get help with financial support and the law.
Funding to help services support victim survivors' needs
-
When giving funding to services, make sure they are focused on providing victim survivors with a good experience every time.
5. Finding your way through the storm
As well as getting help from family violence workers and services, victim survivors might need help to find a new home, get a new job, see a nurse or doctor, or lawyer for court support.
Homelessness services are underfunded … so people are faced with either returning to unsafe situations or sleeping rough either by themselves or with children. – Kelly, victim survivor
As well as getting help from family violence workers and services, victim survivors might need help to find a new home, get a new job, see a nurse or doctor, or to see someone like a lawyer to support them if they need to go to court.
There are now special courts that aim to make it safer and easier for a victim survivor to go to court. These courts have workers who can support victim survivors to figure out what help they need, understand what is happening, and offer support to access a lawyer. They also need to make sure that children and young people who are victim survivors get to have a say where it is safe for them to do so. But some people are not yet getting that chance.
There is a wide range of therapeutic supports available, but it is still very difficult for people to get the support they need, especially for children and young people. There is a need to improve the inclusiveness of services to support people and families from a diverse range of groups such as people who are Aboriginal or Torres Strait Islander, older people, people with disabilities, people who identify as LGBTQIA+, rural and regional communities or migrants and refugees.
Without somewhere consistent and stable to live, it is very hard for people to get back on track. There are not enough affordable housing options available for victim survivors and this is often stopping them from moving from crisis towards stability and recovery.
But what can be done?
We have suggested the following actions for the Victorian Government to tackle these problems (see full list for all 16 suggested actions(opens in a new window)):
Taking a more victim-centred approach
-
Find ways for workers from police, courts, The Orange Door and family violence services to work better together
- Act to make sure that children and young people are seen as victims in their own right and have a say in family violence–related court hearings.
Make sure victim survivors can access the supports they need
-
Make sure that victim survivors can get help with financial support and the law.
Funding to help services support victim survivors' needs
-
When giving funding to services, make sure they are focused on providing victim survivors with a good experience every time.
- Ask for more things that victim survivors need, like housing, help with paying rent and mortgages, help from lawyers about legal problems, financial support and other supports.
More data and monitoring to understand the issue
-
Get better information about how many people are wanting help, and how long it is taking them to get that help.
6. We need care while we are growing
Recovery is not easy and can be a challenging journey. For most victim survivors, recovery and healing requires life-long support through specialised support services.
We need long-term access to mental health supports for victim survivors and their children and the opportunity for stability through stable housing, access to a stable income. Until we have basic needs – like safety, food and shelter – how can we recover? – Jasmine, victim survivor
We know that recovery is not easy and can be a challenging journey. For most victim survivors, recovery and healing requires life-long support through specialised support services – but most people have told us that this is not available.
The support services and system currently focus on the crisis point and the time straight after. While this is very important, there also needs to be more attention and resources for long-term recovery. This would mean more money being put into therapeutic supports so that victim survivors can get help based on their individual needs and can access it when they first reach out for support.
Many victim survivors told us about the importance of connecting with their peers through lived experience groups like the Victim Survivors’ Advisory Council. There should be more platforms available for victim survivors, including specific groups for children and young people to ensure they are seen, partnered with and heard in systems change work.
But what can be done?
We have suggested the following actions for the Victorian Government to tackle these problems (see full list for all 16 suggested actions(opens in a new window)):
Taking a more victim-centred approach
- Keep asking the Australian Government to fix the problems that we know affect victim survivors in the following areas: immigration law, Medicare, Centrelink and the family law system.
Make sure victim survivors can access the supports they need
- Make peer support workers available for victim survivors to help in their recovery.
- Make it clear about how the mental health system works with the family violence system to help support victim survivor recovery.
Support options
If you are concerned for your safety or someone else’s, please contact the police or call Triple Zero (000) for emergency assistance.
We know that young people might have limited access to phone lines due to a lack of privacy or feeling unsafe if they are living with people who might overhear their conversations.
Here are some recommended helplines that also have text or online chat options:
Kids Helpline(opens in a new window) - 1800 55 1800
Free, confidential online and phone counselling service for young people aged 5 to 25 years old. Available 24/7.
1800 Respect(opens in a new window) - 1800 737 732
A national sexual assault, domestic and family violence counselling service. This service is free, confidential and available 24/7.
Lifeline(opens in a new window) - 13 11 14
A national service providing Australians experiencing emotional distress with access to 24-hour crisis support and suicide prevention services. Available 24/7.
Headspace(opens in a new window) - 1800 650 890
A national free confidential online and phone mental health counselling service.
Rainbow Door (Switchboard)(opens in a new window) - 1800 729 367
Switchboard provides peer-driven support services for lesbian, gay, bisexual, transgender and gender diverse, intersex, queer and asexual (LGBTIQA+) Victorians, their friends and family.
Safe Steps(opens in a new window) - 1800 015 188
Free web chat, phone or email family and domestic violence support for people who live in Victoria. Available 24/7
13Yarn - 13 92 76
A support line for mob who are feeling overwhelmed or having difficulty coping. Available 24/7.
Thirrili Postvention Response Service(opens in a new window) - 1800 805 801
The Indigenous Suicide Postvention Response Service supports individuals, families and communities affected by suicide or other significant trauma. Available 24/7.
InTouch(opens in a new window) - 1800 755 988
Specialist family violence provider supporting migrant and refugee women and their communities experiencing family violence. Available Monday to Friday, 9:30am - 4:30pm.
Victims of Crime Helpline(opens in a new window) - 1800 819 817
Service offering free information and support for people affected by crime. Available from 8am to 11pm, seven days a week.
Definitions
Words that are bolded in this summary are explained in this definitions page.
| Crisis | This can mean different things for different people. For some, this may be the point where they are in a time of intense difficulty or danger, and they need help quickly to protect themselves. But for others, this may be when they first reached out and asked for help. |
|---|---|
| Family violence |
Family violence looks different for everyone. It could be a parent, sibling, relative, someone you’re in a relationship with, who you live with, or used to live in your home (for example, a parent’s ex-partner) who uses violence. Family violence can look like hitting, punching, screaming, threatening, speaking down to, controlling behaviours and getting people to do sexual things they don’t want to. It could also look like hearing, seeing or being around the impacts of violence. It may leave people feeling scared, unsafe, alone, and physically hurt. These are just some of the ways people can experience family violence. |
| Family violence worker | A professional that works with victim survivors to understand risk, help them create a safety plan, link in with other support services, and someone they can talk to. |
| Implementation | The process of putting a decision or plan into action. |
| LGBQTIA+ | An abbreviation for lesbian, gay, bisexual, queer/questioning, transgender, intersex and asexual. These terms are used to describe someone’s sexuality or gender identity. |
| Lived experience | In this summary, lived experience is a deep knowledge that is held by someone who has been through or still surviving family violence. |
| Peer Support Worker | A peer support worker is someone who has been through hard times like family violence and mental health challenges. They provide emotional and social support and hope to others and help us know that we are not alone in what we are going through. |
| System | A system is a collection of parts that aim to work together. The family violence system includes Child Protection, Police, Courts, The Orange Door, justice and legal, family violence services and education to help and support victim survivors with their needs at the point of crisis, and through their journey towards recovery. |
| The Orange Door | A free service for adults, children and young people who are experiencing or have experienced family violence. It is a place where victim survivors can go to get help. They also connect people who use violence with the services they need. |
| Therapeutic services | Are made up of professionals and specialised ways of working that provide help or support to victim survivors to feel better about themselves and their future. |