
There are very clear entry points into the family violence service system for most victim survivors seeking help: Victoria Police, The Orange Door and the Safe Steps Family Violence Response Centre. It is a great achievement that awareness of what family violence is and where to go for assistance appears to be increasing. However, likely because of that awareness, demand pressure continues to increase (see Figure 4 and Figure 5), and we heard numerous accounts of victim survivors experiencing long waits to have their risk and needs comprehensively assessed at The Orange Door, except in the most serious cases. Furthermore, some groups of victim survivors face additional barriers to linking in with the family violence service system.
There are some clear areas for improvement, including the need to streamline intake and assessment processes at The Orange Door, reconsider the service pathway for male victim survivors, and more effectively communicate with groups that may be more likely to self-exclude from The Orange Door and the family violence system more broadly.
Figure 4: Family violence incidents recorded by Victoria Police

{kind=link}
Police response and referrals
Victoria Police has comprehensive guidance in place for members responding to family violence incidents. This guidance is captured in the Victoria Police Manual: Family Violence, Code of Practice for the Investigation of Family Violence, and a range of practice guides. Victoria Police’s Family Violence Options Model, contained in the code of practice, clearly articulates that the actions taken should aim to support: safety for adult and child victims, appropriate referrals being made, the prevention of future family violence, and investigation and prosecution of perpetrators where appropriate.
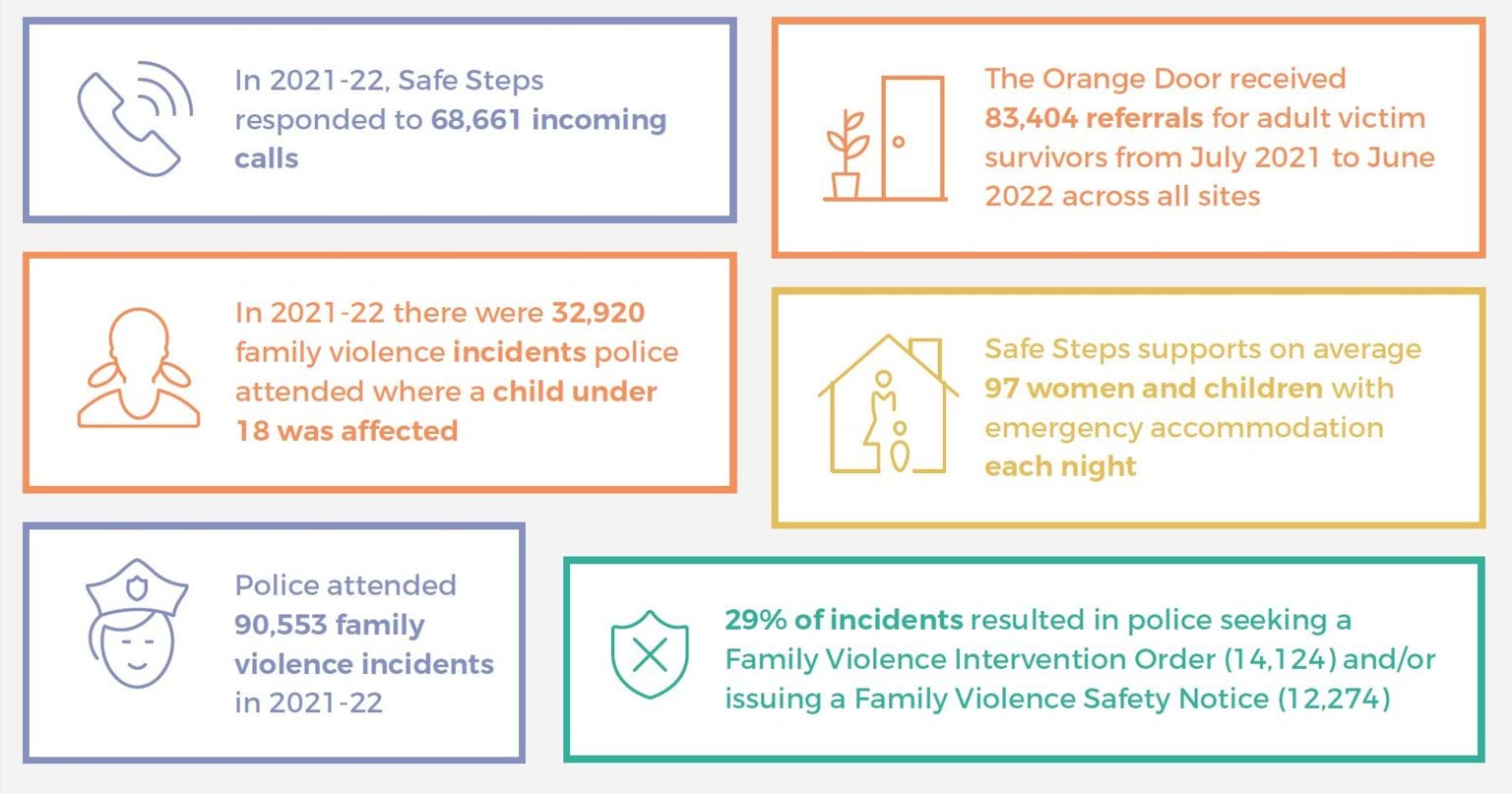
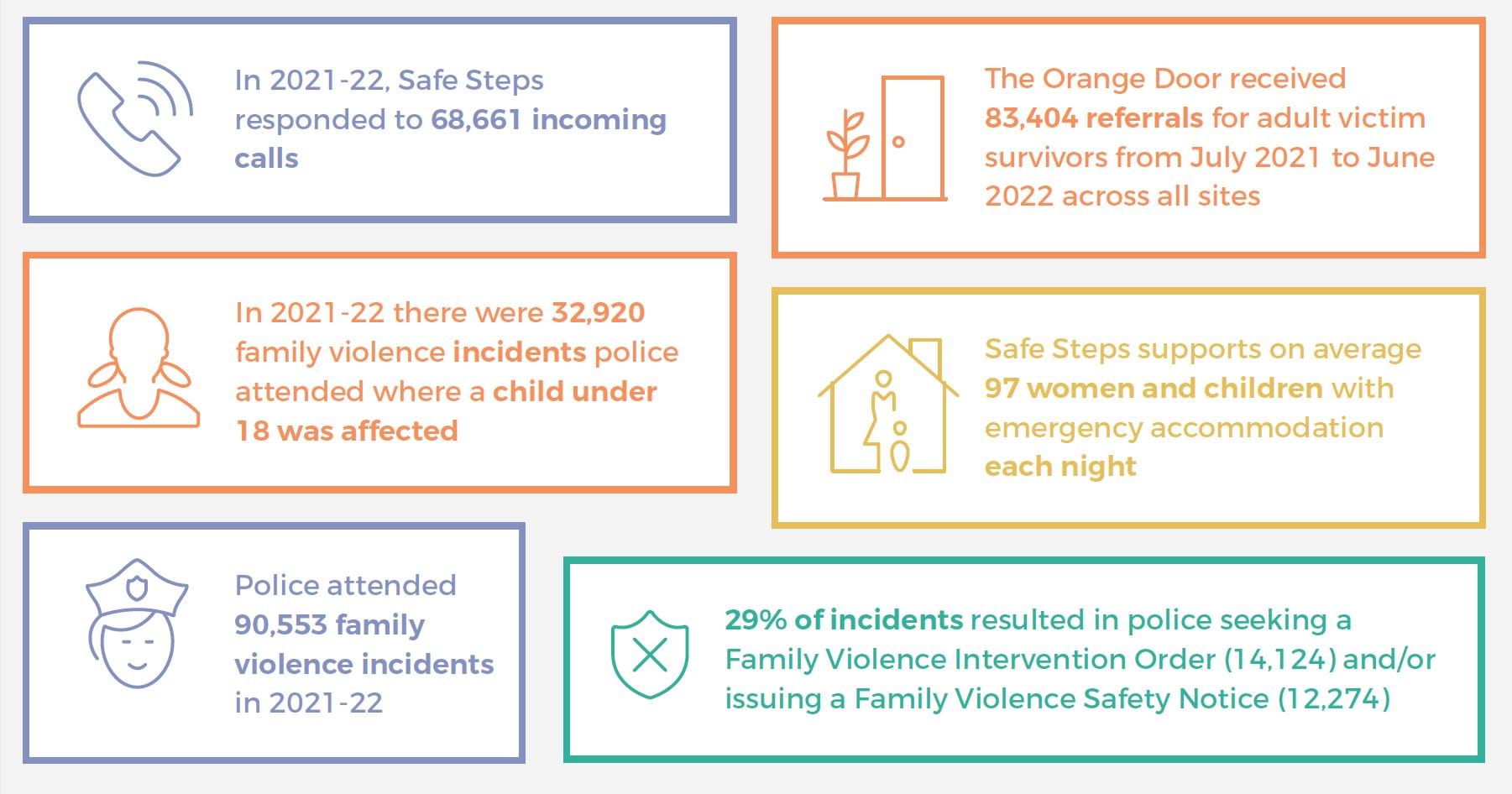
Figure 5: Highlighted statistics demonstrating the need for family violence support
{kind=link}
Child safety is a priority in the guidance, with the Victoria Police Manual being clear that members are expected to assess the interests of the child independently of a parent. Police members are also expected to respond effectively to the diverse needs of priority populations, with the Family Violence Priority Community and Diverse Community Responses practice guide outlining, among other things, barriers to reporting and recommended police practice for engaging with a number of priority groups in the community. The code of practice is clear that ‘Victoria Police recognises the importance of an intersectional approach when responding to and investigating family violence across our diverse Victorian community’.
Family violence and Child Protection referrals are also clearly described in police materials:
- Referrals to family violence services are automated through the Family Violence Report (L17) portal, where there are immediate concerns for the safety and welfare of victim survivors. Alternatively, where there are no immediate concerns, victim survivors are provided with information on who they can call, as part of an ‘informal referral’. Formal referrals appear to be far more commonly used, however, with 81,048 formal referrals for affected family members across all police regions in 2020–21, in contrast with 10,785 informal referrals.1
- Mandatory reports to Child Protection are required ‘as soon as practicable after forming a belief on reasonable grounds that a child has suffered or is likely to suffer significant harm as a result of physical injury or sexual abuse, and the child’s parents are unable or unwilling to protect the child’.2 Members are also asked to consider reporting to Child Protection where children have suffered or are likely to suffer significant harm as a result of other forms of abuse or neglect. In 2020–21 police attended 33,948 family violence incidents involving children (7,834 incidents where a child was recorded as the affected family member and 27,639 incidents where a child was recorded as witnessing family violence).3 In the same year, police made 4,098 direct referrals to Child Protection and 6,942 direct referrals to Child FIRST.4 In addition, where a formal referral via the L17 portal is made but the threshold for a direct referral to Child FIRST or Child Protection is not met, the specialist family violence services and the Victims of Crime Helpline receiving the formal referral will consider the need for children involved to be referred, and will make referrals if appropriate. There are multiple opportunities for referral to Child Protection and Child FIRST, and children may also receive support through family violence, therapeutic and other services, but as discussed throughout this report, gaining access to these services can be difficult, and we are concerned that many children experiencing family violence may not be receiving direct support at all.
- Victoria Police has a separate e-referrals system for referrals to other services including legal, youth and mental health services. It is not clear how often such referrals are made.
While Victoria Police guidance is comprehensive, practice that matches the strategic intent does not always occur, as discussed in detail in our Accurate Identification of the Predominant Aggressor report. Stakeholders including Victoria Police and the Coroners Court of Victoria explained that public expectations of police responses to family violence are increasing, while the number of family violence incidents is also on the rise. To address this challenge, one model that has been suggested and trialled in some locations is a co-responder model, whereby a social worker attends family violence incidents together with police. Once such model is the Alexis – Family Violence Response Model, which was co-designed by Victoria Police and The Salvation Army, in collaboration with other local stakeholders. It involves an Alexis Senior Family Violence Practitioner from The Salvation Army being physically located within the local Victoria Police Family Violence Investigation Unit, and provides a coordinated, multi-agency response to families who are having repeated contact with police and services due to family violence. The initiative has been evaluated and shows promising results, including a reduction in family violence incidents for families receiving the Alexis response, and vastly improved victim survivor engagement with social services (see Box 1 for an example). As the Coroners Court of Victoria told us:
Given the ongoing challenges faced by the sector in providing victims of family violence with an appropriate response, the State Coroner is currently exploring whether the expectations placed on police when responding to family violence are realistic and how victims may be better supported to engage in family violence services. As a part of this consideration, the State Coroner is working with the [Victorian Systemic Review of Family Violence Deaths] Review Panel to explore the benefits and utility of a state-wide co-responder model.
We would support such exploration and suggest it may be a way to ensure improved engagement of victim survivors with the family violence service system, who may not otherwise engage following police attendance at an incident, despite any referrals made [relates to action 2].
Box 1: The Alexis-Family Violence Response Model in action
Roxy was a 47-year-old inpatient at a public hospital being treated for breast cancer in 2021. The hospital Roxy was attending systemically responds to family violence - including actively using MARAM and information sharing provisions - with the support of the Strengthening Hospital Responses to Family Violence initiative. Hospital staff referred Roxy to the local Victoria Police Family Violence Investigation Unit (FVIU) because she was facing a range of challenges, including physical and mental ill-health (with a history of suicide attempts), unstable and transient housing, and disclosures of family violence. Roxy was still in a relationship with the perpetrator and was experiencing ongoing physical, psychological and financial abuse and controlling behaviours. The FVIU that received the referral included co-located specialist family violence practitioners from The Salvation Army under the Alexis Family Violence Response Model.
The intervention commenced with police and Alexis workers attending the hospital jointly to meet with Roxy, who detailed her background, relationship history, current concerns and stressors. Roxy was not initially seeking formal intervention by police but was receptive to ongoing informal police support and assistance from Alexis workers with her self-identified ultimate goal of separation from the perpetrator.
Throughout the duration of the support period, a care team approach to intervention was taken, bringing together Alexis practitioners, police, housing support, hospital staff and mental health services. Collectively, the care team provided support such as:
- psychoeducational and emotional support around family violence
- risk management planning, conducted at the hospital directly after cancer treatment sessions, to avoid the perpetrator knowing about them
- completion of a Victorian Housing Register application for social housing
- police and legal advocacy around the Family Violence Intervention Order process
- support to re-establish relationships with estranged family members
- support with re-entering education.
Seven months after referral, Roxy was in remission following surgery and cancer treatment. Her mental health was reported to be currently stable. She had separated from the perpetrator and a three-year Family Violence Intervention Order had been put in place. Roxy was in women’s supported accommodation and she was expected to shortly receive ongoing housing. Roxy has since reconnected with family members and re-entered education to pursue a career in mental health peer support.
Source: Based on a case study provided by The Salvation Army.
Crisis response model
Building on the previous after-hours response model, Family Safety Victoria has developed a crisis response model in consultation with the sector. The model is now finalised, approved and being distributed across the sector, and alignment is expected by 1 April 2023. The model is captured in three documents:
- the Case Management Program Requirements (discussed in the next section)
- Roles and Responsibilities After Hours
- Role and Responsibilities in Providing Emergency Accommodation.
According to the Case Management Program Requirements, a crisis response is an ‘urgent, rapid intervention to mitigate risk and harm for victim survivors’. This response is for victim survivors identified to be at serious risk of harm and with urgent safety needs. A crisis response can be initiated by Safe Steps, The Orange Door or a local specialist family violence service, although Safe Steps offers an all-hours service. Child Protection also delivers an all-hours service to respond to children and young people at risk, including those facing an immediate risk of harm due to family violence.
Safe Steps responds to any victim survivor who calls seeking help through its all-hours phone line or live chat support, providing, at a minimum, risk assessment and safety planning. Safe Steps responded to 68,661 calls in 2021–22, with an average time on hold of approximately two minutes. This suggests that despite significant demand, victim survivors who are calling for help are getting to speak to a specialist family violence practitioner promptly.
As might be expected, stakeholders told us that victim survivors with the most urgent needs are receiving the timeliest and most effective responses from the service system. Where victim survivors face an imminent threat, various parts of the system (including, for example, Victoria Police, Safe Steps, The Orange Door and crisis accommodation services) work together to swiftly get the victim survivor(s) to safety.
Despite the positive feedback, there are some very real challenges for staff providing crisis responses to victim survivors in immediate danger. One challenge is the incompatibility of information systems being used by different parts of the system. For example, The Orange Door and Safe Steps use different client management systems, so when a crisis response transfers from The Orange Door during business hours to Safe Steps for an after-hours response, information has to be manually handed over, or risk assessments have to be repeated.
Another challenge is finding appropriate emergency accommodation. A refuge eligibility and prioritisation framework has been developed to clarify how applications for refuge should be prioritised and confirm a central coordinating role for Safe Steps. This will likely be helpful in making prioritisation decisions; however, the vast majority of victim survivors will not be able to access refuge at all. We heard that many victim survivors are in crisis but don’t meet the urgency criteria for refuge accommodation, yet if they seek general homelessness support, they are told they need a crisis response. For young people fleeing violence on their own, we were advised that there are very few options.
Many stakeholders, including victim survivors, said that clients with alcohol and other drug (AOD) issues are told they must be ‘clean’ for six weeks before they can receive crisis accommodation. Through the Victorian Alcohol and Drug Association, we also received numerous examples of clients using alcohol and/or other drugs (some of whom are coerced to do so by their perpetrator) being denied a crisis response service and adequate protection through the family violence system, despite risk being identified by AOD clinicians. We suggest there is room to improve the capability of the family violence system for clients who use AOD to ensure they can access appropriate support.
The excess demand for refuge places has led to a reliance on motel accommodation. For example, Safe Steps has advised that in 2021–22 it accommodated 3,124 unique clients, and despite 72 per cent being classed as ‘serious risk’ or ‘serious risk requiring immediate protection’, 90.8 per cent of cases were accommodated in motels. The use of motels has been widely criticised,5 but in the absence of any other options, it has become a necessity. The new crisis response model appears to begin to respond to past concerns (which were reflected in our 2020 report) about victim survivors accommodated in motels being insufficiently supported. The model aims, in part, to ensure all victim survivors in emergency accommodation have access to face-to-face support from a specialist family violence service and are supported in their transition out of emergency accommodation. However, the Statewide Family Violence Integration Advisory Committee remains concerned about:
…. increasing numbers of women and children residing in inappropriate and unsustainable crisis accommodation … for extended periods of time with only ‘brief intervention’ support whilst awaiting specialist family violence case management allocation.
Although more work is required, substantial efforts are being made to improve the suitability of emergency accommodation options for victim survivors. For example:
- The Refuge Redevelopment Program is replacing 17 communal refuges with ‘core and cluster’ designs and constructing another three Aboriginal-designated refuges. There have been some implementation delays due in part to COVID-19 and rising costs of building materials, but as of 8 November 2022, 13 of the sites had been completed and handed over to agencies. The core-and-cluster design is more suitable for families and women with disabilities. However, as Women with Disabilities Victoria pointed out, for example, the low benches that have been installed in some of the units to support those requiring them are not height adjustable and therefore won’t suit a range of needs. We suggest ongoing engagement between government and the agencies delivering the refuge services to identify areas for improvement and refinement.
- The Motels Coordination Initiative is a year-long initiative that began in June 2022. It is working to identify and address key issues with using motels (or other private accommodation) as emergency accommodation. The initiative acknowledges that while motels are an option of last resort, their use is required to meet excess demand. The initiative is driven by funded Local Family Violence Motel Coordination Projects in each of the 17 Department of Families, Fairness and Housing areas, which aim to identify local area solutions and opportunities for improvement, and a Statewide Reference Group, which is responsible for considering more strategic responses to issues and making recommendations.
- Safe Steps and Safe and Equal have developed advice for services providing crisis responses to guide relationship management with moteliers and to identify preferable emergency accommodation characteristics.
Another important part of the crisis model is brokerage funding. During consultations for this report, as well as for past reports, stakeholders have spoken about the benefits of being able to mobilise brokerage funding for victim survivors to promptly and flexibly access supports to meet their needs. Currently, we are aware of three such sources of brokerage that can be used to support victim survivors to transition out of crisis: flexible support packages, crisis brokerage and the Disability and Family Violence Crisis Response Initiative (DFVCRI). The DFVCRI, which we are advised has ongoing funding, is accessible through Safe Steps’ family violence specialist disability liaison officers and is pivotal in allowing the system to meet the urgent needs of victim survivors with disabilities seeking safety from family violence situations. This is because the National Disability Insurance Scheme cannot provide responses to immediate disability-related crisis needs. Safe Steps and Women with Disabilities Victoria have advised that there is considerable room for improvement in ensuring more people are aware of the initiative so it can be more widely used.
The Orange Door
The Orange Door network is now operating in all 17 Department of Families, Fairness and Housing areas in Victoria, so no matter where a person lives in the state, they can access support through The Orange Door. Looking at data from the past year, referrals and presentations to The Orange Door have remained relatively consistent over time, given the increasing number of sites (see Table 1).
Table 1: Referrals for children and adult victim survivors to all active The Orange Door locations, July 2021 to June 2022
| Month | Jul | Aug | Sep | Oct | Nov | Dec | Jan | Feb | Mar | Apr | May | Jun |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Child referrals* | 5253 | 6389 | 6029 | 6027 | 8570 | 8493 | 7296 | 8700 | 10118 | 8690 | 10240 | 10004 |
| Adult victim survivor referrals | 4578 | 5019 | 5212 | 5555 | 7281 | 7750 | 7222 | 7690 | 8685 | 7457 | 8785 | 8170 |
| Number of sites operating | 8 | 9 | 10 | 11 | 13 | 13 | 13 | 14 | 14 | 14 | 15 | 15 |
*Child referrals include children referred for family violence reasons and/or wellbeing concerns. During this period, approximately 20 per cent of children referred to The Orange Door proceeded to the assessment stage and were found to be victim survivors.
Source: Data provided by Family Safety Victoria.
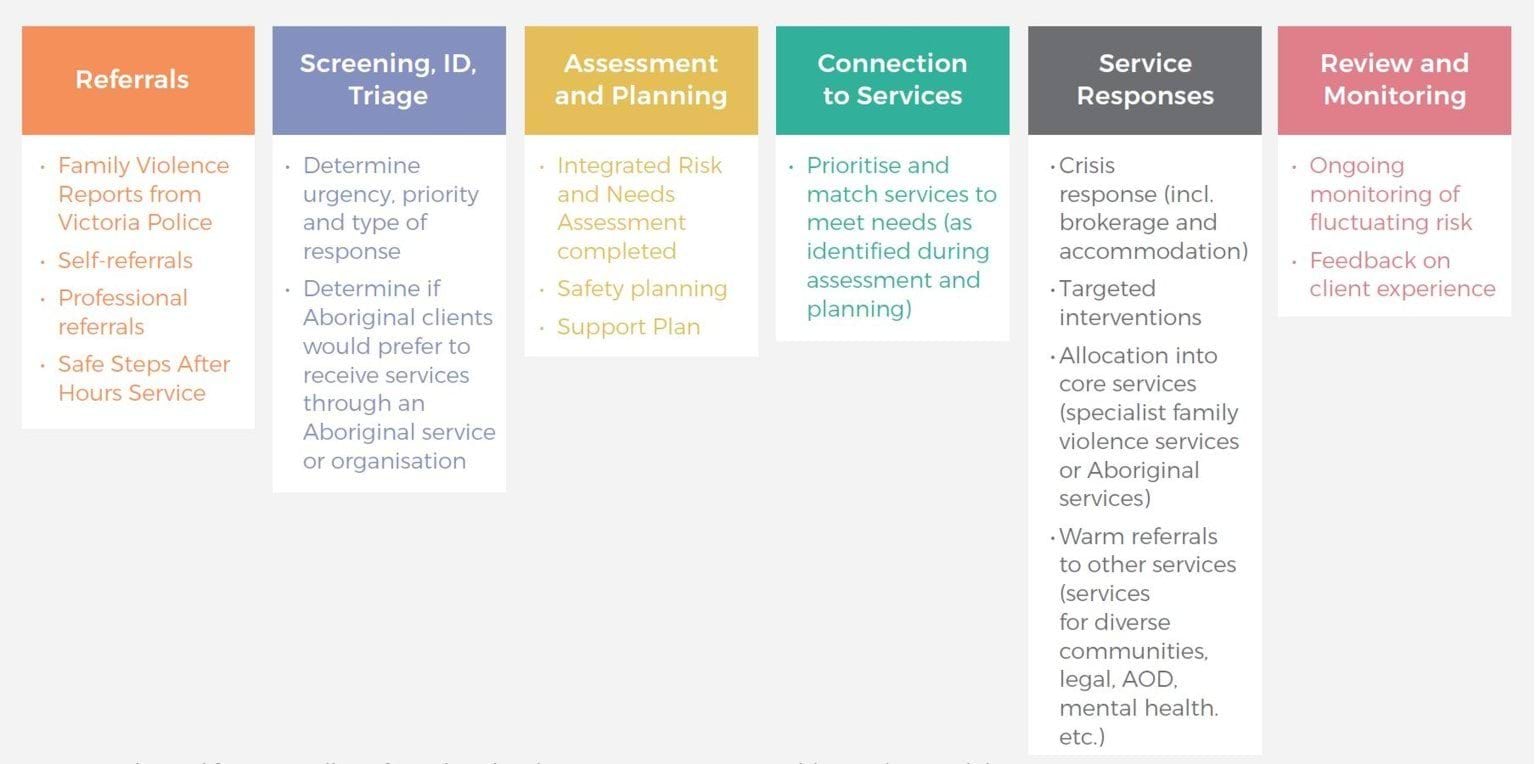
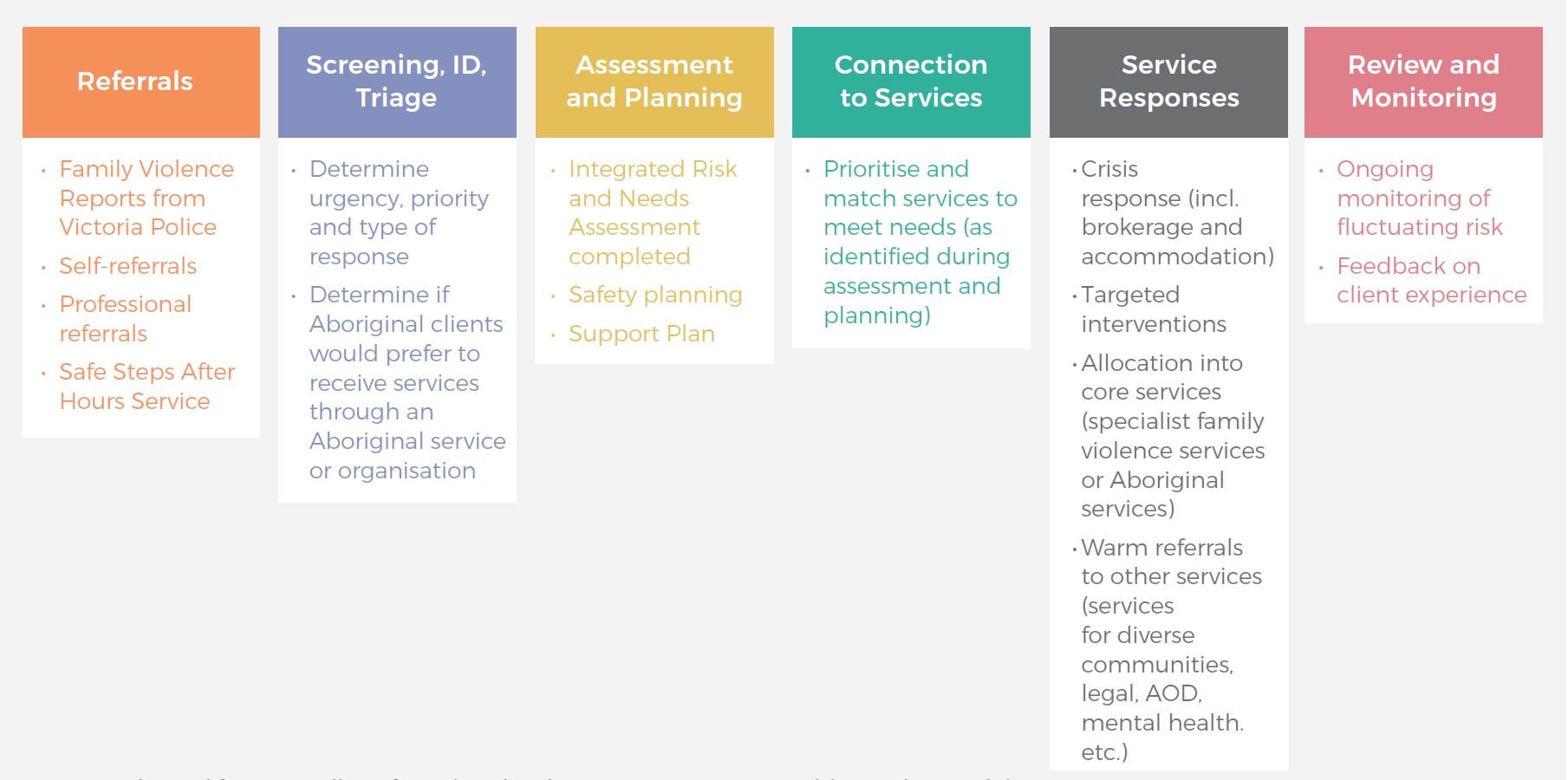
Based on our consultations, there was broad support for The Orange Door model and its potential to ensure a clear and consistent process for intake into the family violence service system. Indeed, we were highly impressed by The Orange Door practitioners we met across multiple sites during this monitoring period. They spoke with a great deal of expertise, understanding of the key challenges and commitment to improving the way victim survivors’ safety and wellbeing could be supported. As it has been described to us, The Orange Door service model is logical, thorough and designed to prioritise victim survivors at greatest risk (see Figure 6). In practice, however, multiple stakeholders have raised issues and areas for improvement. These are explored below.
Figure 6: The Orange Door service model
{kind=link}
Most commonly, stakeholders spoke about processes within The Orange Door taking much longer than expected, leading to bottlenecks in victim survivors being able to access case management support from specialist family violence services. It is difficult to get a very clear picture of the extent of these delays and what is causing them [relates to action 14]. The data we have seen shows that triage (which involves checks of the available databases to look at the pattern and history of violence) occurred, on average, within three and a half days during 2021–22. The average wait time between referral and having a case worker assigned was 11.8 days across April to June 2022 (see Table 2). More detailed investigation would be required to explore wait times for assessment and whether there are particular groups for whom delays are more common [relates to action 16].
Table 2: Triage priority for child and adult victim survivors, and average wait times
| Tier (as determined at assessment stage) | Proportion of victim survivors | Average time from referral to triage finalisation - ADULT | Average time from referral to triage finalisation - CHILD | Average time from referral to assessment - ADULT | Average time from referral to assessment - CHILD |
|---|---|---|---|---|---|
| Tier 1 | 65% | 2.7 days | 3.2 days | 8.4 days | 8.5 days |
| Tier 2 | 27% | 4.4 days | 4.3 days | 18.2 days | 14.8 days |
| Tier 3 | 8% | 3 days | 3.6 days | 10.8 days | 10.8 days |
| All tiers | 100% | 3.4 days | 3.6 days | 11.3 days | 10.3 days |
Note: Tier 1 is the highest priority. Time to triage finalisation based on the average from July 2021 to June 2022. Time from referral to assessment (where client is assigned a worker) is based on the average from April-June 2022.
Source: Data provided by Family Safety Victoria
We were also frequently told that there is considerable variation across The Orange Door sites – that ’every site does it differently’. While some local variation is to be expected, a key aim of The Orange Door is to ensure greater consistency of response wherever a victim survivor accesses the service system.
While we understand that The Orange Door accepts all victim survivors, many victim survivors and third-party professionals we have spoken to this year reflected experiences where victim survivors are referred to The Orange Door but ultimately do not meet the threshold for support, leaving them feeling discouraged. Further investigation is required to determine where this perception of a ‘threshold’ is coming from.
The Orange Door is also explicit about wanting to offer ‘accessible, responsive and non-discriminatory supports tailored to individual needs and experiences’; however, some victim survivors are reluctant to access The Orange Door. For example, we were told that older people experiencing family violence will usually see The Orange Door (and family violence services more broadly) as being for younger women and children and will self-exclude. Many stakeholders raised the presence of Child Protection within The Orange Door as being a deterrent to some victim survivors reaching out to the service. This was particularly relevant for Aboriginal clients and clients with a disability, who had heightened concerns about potentially having their children removed from their care, although we note that these concerns existed even before the introduction of The Orange Door model. It is, therefore, important to continue to build trust and capability within mainstream family violence services (see, for example, Box 2) to better respond to diverse needs, and to support all services, including by having a clear approach to referrals, secondary consultations and coordination [relates to action 1]. For example, several Aboriginal Community Controlled Organisations advised that mainstream services working with Aboriginal clients do not consistently seek secondary consultations or share information with them. The Victorian Aboriginal Child Care Agency has indicated that more work is required to improve the response system to ensure services are culturally safe, and it recommends that minimum standards on cultural safety for the mainstream sector are developed, implemented and reported on.
Equally important is the need to retain the ‘no wrong door’ approach that effectively links victim survivors with support wherever they feel comfortable accessing the system (for example, The Rainbow Door, Seniors Rights Victoria and Aboriginal Access Points). Many Aboriginal Community Controlled Organisations spoke of the need for improved data about family violence and its links with other issues within their communities, to inform stronger planning for self-determined, holistic service delivery.
Box 2: Case example: establishing risk with a victim survivor with a disability
Maggie presented to The Orange Door seeking family violence support. She has a cognitive disability, and in her initial risk assessment, Maggie reported that her partner Stephen was mean to her dog, and that he would take the dog outside and tie him up. This was noted in her original referral report with no further context.
Due to her disability, The Orange Door referred Maggie to a private practice family violence consultant. Maggie had a number of sessions with the consultant, where the consultant built trust and was able to take the time and find ways to communicate appropriately with Maggie.
During the fourth session with the consultant, it was established that the dog was actually an assistance animal for Maggie, not just a family pet. The consultant also elicited that when Maggie said Stephen was ‘mean to the dog’ and being ‘tied up’, he was actually tying the dog upside down by its feet and hitting it. Maggie also revealed that this was often in response to Maggie refusing demands for sex, or to get her to agree to sex with the threat of hurting the dog.
This information changed the risk assessment of the level and types of violence against Maggie significantly. Had the consultant not developed the shared communication understanding and taken the extra time with Maggie, she may not have been referred to the appropriate supports needed to recover from her family violence experiences.
Source: Adapted from information provided by Women with Disabilities Victoria.
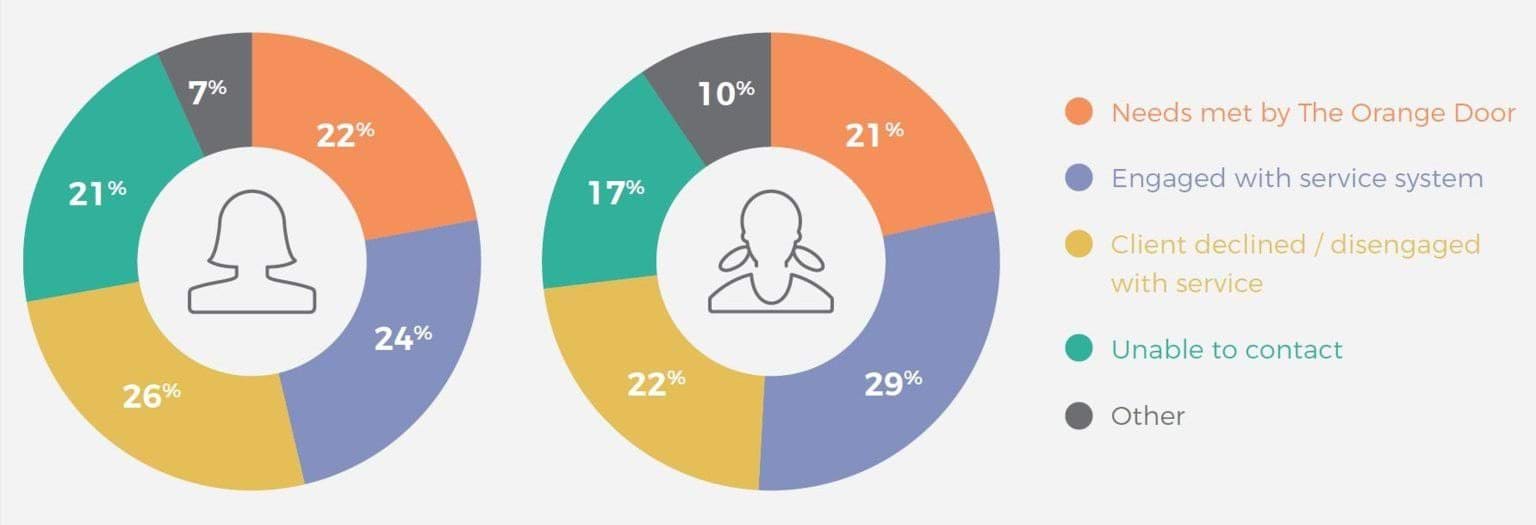
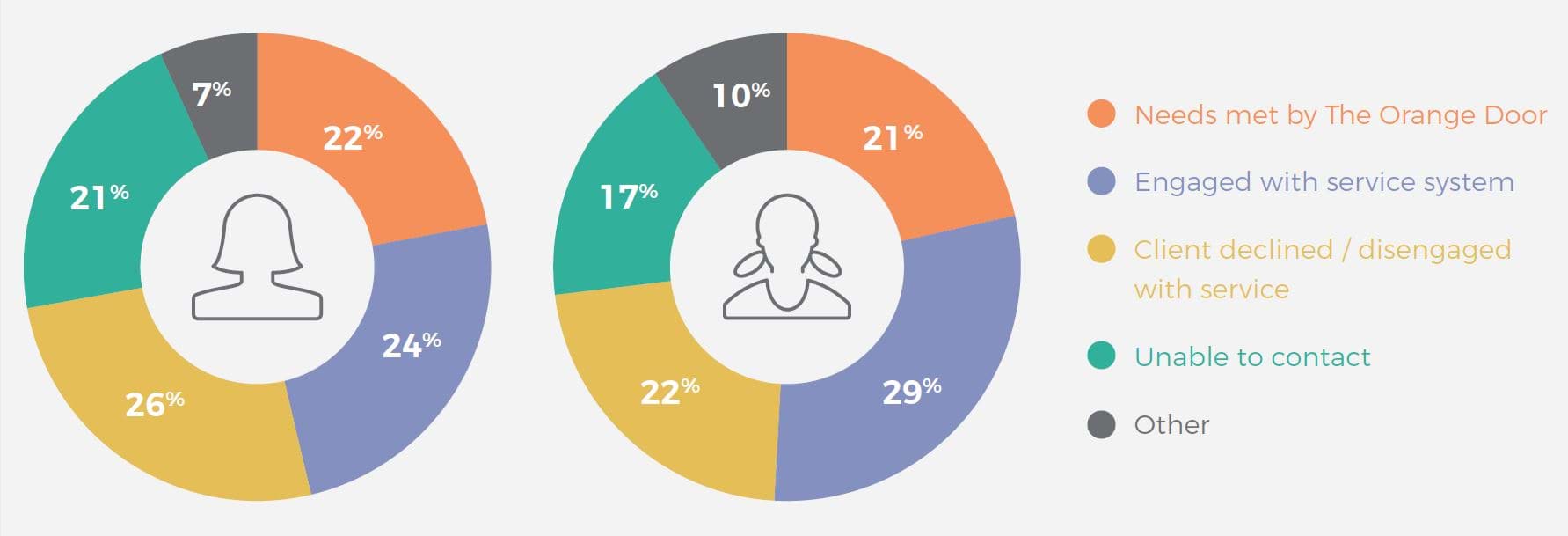
We note that significant proportions of victim survivors are either unable to be contacted or are declining service from The Orange Door (see Figure 7). While acknowledging that The Orange Door is a voluntary service and victim survivors may legitimately choose not to engage, it may be worth exploring this further, particularly the ‘unable to contact’ group.
Figure 7: Victim survivor case closures across The Orange Door locations, by reason
{kind=link}
The implementation of The Orange Door model is an ongoing process, with many sites still very new. As implementation continues, so too must refinement of the model, based on ongoing monitoring. The findings from case file audits will be of great benefit here because they ‘provide insights into the quality of the work that is undertaken with clients and how that work is documented on the case-file’. Systematic case file audits occur three times per year at each site in The Orange Door network. They are carried out by local leadership teams and a findings and recommendations report is prepared and shared with Family Safety Victoria to ensure visibility of issues that may be of system-wide significance. Targeted case file audits can also occur at the discretion of each site’s Hub Leadership Group. While this is an important part of the ongoing monitoring and continuous improvement of practice in The Orange Door, we suggest the following is also required to be able to adequately explore and address the issues we have raised in this section:
- greater central visibility of practice across The Orange Door network by Family Safety Victoria (for example, by establishing an internal review function) [relates to action 16]
- active consideration of timeframes for clients moving through The Orange Door and whether wait times could be improved by streamlining processes [relates to action 14]
- engagement of client voices, including their expectations and experiences of The Orange Door
- analysis of client journeys through The Orange Door and into the service system. Such analysis will be challenging because various parts of the system are using different client management systems, so work to better align these systems over time will also be essential [relates to action 15].
Process for male victim survivors
Of all affected family members (victim survivors) identified by Victoria Police at family violence incidents in 2020–21, 25 per cent were male (22 per cent were males over the age of 18). Notwithstanding the very real issue of some men being misidentified as victim survivors, as explored in our Accurate Identification of the Predominant Aggressor report, there are genuine adult male victim survivors requiring support. Family Safety Victoria has advised that male victim survivors who contact The Orange Door for assistance can be directly supported. Male victim survivors can also contact Safe Steps and receive support, including family violence risk assessment and safety planning in urgent cases. We understand that accommodation options for male victim survivors are very limited, though, and usually rely on the broader homelessness system.
However, in general, adult male victim survivors of family violence have a different pathway into the system. The Victims of Crime Helpline, operated by the Department of Justice and Community Safety, is the main gateway for adult males requiring further support to respond to their experiences of family violence. Male victim survivors identified by Victoria Police through a Family Violence Report are automatically referred to this helpline. Helpline staff can support victim survivors with risk and needs assessments and safety planning, and can refer them on to the Victim Assistance Program (discussed in the next section). Male victim survivors constitute a significant proportion of calls and referrals to the helpline. For example, in 2019–20, 10.7 per cent (1,512) of inbound calls were for male victim survivors of family violence, and 65.7 per cent (17,369) of referrals were from Victoria Police for male victim survivors.
Concerns have been raised about this referral pathway: in particular, that the helpline is a generalist rather than specialist service, and that there is a lack of appropriate referral options. As explained by the Centre for Innovative Justice in its 2020 report on the victim support system:
The current Male L17 Response comprises more than 50 per cent of Helpline referrals but is not supported by a dedicated workforce or specialised response. This is despite recognition among the broader family violence sector that this is highly complex work, including involving predominant aggressor assessments. Further, responding to male victims of family violence represents unique challenges given the lack of services available to this cohort, and the stigma and shame which male victims of family violence may experience.
The centre suggested that, to address this, a dedicated male victim survivor response be established within the helpline to provide more specialised support. It may also be worth considering whether a new pathway to family violence services should be created for adult male victim survivors [relates to action 8]. For example, although The Orange Door and specialist family violence service can and sometimes do support male victim survivors presenting to them, the practice of referring male victim survivors onto a separate referral pathway can create confusion for the public about where to seek support and can come into conflict with the work of the sector to be more LGBTIQ+ inclusive.
Footnotes
- Crime Statistics Agency, Victoria Police Data Tables 2020–21. Table 18: Referrals made by Victoria Police by Police Region and Sex of the Affected Family Member, July 2016 to June 2021
- This is a requirement under the Children, Youth and Families Act 2005.
- Crime Statistics Agency, Victoria Police Data Tables 2020–21. Table 15: Family Incidents Involving Children, July 2016 to June 2021.
- Crime Statistics Agency, Victoria Police Data Tables 2020–21. Table 18: Referrals made by Victoria Police by Police Region and Sex of the Affected Family Member, July 2016 to June 2021.
- For example, Women’s Housing Alliance (2020): Media release: Alliance of women’s housing providers calling for increased funding for the sector, 7 March 2020.
Updated