
The Royal Commission identified three pillars of recovery – secure and affordable housing, financial security, and health and wellbeing – and highlighted the need for adequate support in each of these areas to help victim survivors rebuild their lives. Support available in these pillars has been covered throughout this report, but as has already been raised, there are substantial issues in the capacity of these services to meet demand and provide support in a coordinated way to meet an individual’s needs. Support is also often time-limited, which many stakeholders told us does not reflect the needs of victim survivors over time. There is a need for longer term models of support to allow victim survivors to heal, which likely needs to
include a defined role for the health and mental health systems, and peer support.
Importance of long-term support
The National Plan to End Violence Against Women and Children 2022–2032 recognises that ‘recovery and healing takes time and victim-survivors will, in many cases, require life-long support through dedicated and tailored services and interventions’. Yet one of the pieces of feedback we most consistently received during our consultations was that a clear crisis to recovery model has not been articulated. Powerfully, the CEO of Safe and Equal told us that:
The system has never been funded for recovery. We know that recovery is a long journey, and it is not linear or predictable. We need to continue to build the evidence base for what supports long term recovery, but at the very least, we need investment in the system for ongoing therapeutic supports so that victim survivors can access a range of options based on their individual needs, when they need it.
Similarly, Djirra said:
There is no talk about what [recovery and support] looks like over the lifetime … no ongoing holistic recovery from trauma, especially intergenerational trauma; it doesn’t exist at all.
This affects the ability of services to provide the long term support that victim survivors need. Djirra noted that this is particularly relevant to Aboriginal services:
Aboriginal services are working with women who have complex and often multigenerational trauma and require long term and specialised support for themselves and their families.
The system is said to be geared towards crisis and the period immediately afterwards. While this is somewhat understandable in the context of overwhelming demand, it means there is likely an insufficient focus on recovering from the trauma of family violence, and victim survivors often feel prematurely disconnected from support. Ironically, cutting support short for victim survivors because of demand pressure may result in victim survivors returning to the perpetrator, ending up in similar relationships in the future and/or continuing to struggle with the ongoing negative impacts of family violence, thereby increasing the level of support they are likely to need in the future. For some victim survivors, the family violence may continue for many years, even after separation, such as in cases where there is shared custody of children.
We heard a number of examples that illustrate the types of longer term support that might be effective:
- One victim survivor was extremely grateful for a sexual assault service worker who she said helped give her a sense of hope and empowerment. With the support of the worker, the victim survivor was able to consider her own strengths, skills and knowledge and use this to get a job and regain control of her life.
- Another victim survivor experienced depression and anxiety during pregnancy and had the support of PANDA (Perinatal Anxiety & Depression Australia). The service called her weekly throughout the pregnancy, just to check in, and the victim survivor said she found this extremely supportive and an important way to be connected with other services when she was not okay. She wonders if a similar model could be applied to family violence.
- The sexual assault service sector was said to be better at recognising the need for victim survivors to be able to reconnect with a service over time as life events trigger past trauma. For example, the Goulburn Valley Centre Against Sexual Assault explained that it is funded to deliver support across a person’s lifetime, and that it is very common for victim survivors to transition in and out of the service over many years depending on their needs. Stakeholders noted that the family violence system does not work in this way, although the call for funding submissions to deliver therapeutic family violence services does indicate a similar model:
Recovery from family violence can take a long time for some victim survivors whose support needs may fluctuate and change through the sustained healing process. Everyday life events have the potential to negatively trigger a victim survivor who may require re-engagement with services. It is important that clients know that when they leave the service that they are still supported by the provider and can seek further assistance in the future, whether through a service offered by that provider or through referral to another one (in the broader sector) that can best fit their needs.
- McAuley Community Services for Women spoke about the value of the simple act of periodically hosting lunches where any client, past or present, can attend, reconnect with the service and chat with other victim survivors.
Ongoing role of the health sector
The call for funding submissions to deliver therapeutic interventions included a section on ‘transition to community support and sustained support’, stating that ‘the purpose of the transition process is to ensure clients have sustained and ongoing support as they continue on their recovery process’. Successful providers were required to either plan to support clients’ ongoing therapeutic recovery after an intervention or ‘demonstrate the process for transitioning clients to sustainable recovery pathways’. One likely source of ongoing support is the broader health and mental health sector [relates to action 7].
According to the 2017 Victorian Population Health Survey, 66.7 per cent of women and 36.4 per cent of men who experienced family violence had been diagnosed by a doctor with depression or anxiety (see Figure 16), compared with 31.3 per cent of women and 20.7 per cent of men who did not experience family violence. However, victim survivors have expressed that the mental health system is not working for people from low-socioeconomic communities or with complex trauma, with access to free services subject to excessively long waitlists.
Figure 16: Victim survivors diagnosed with depression or anxiety
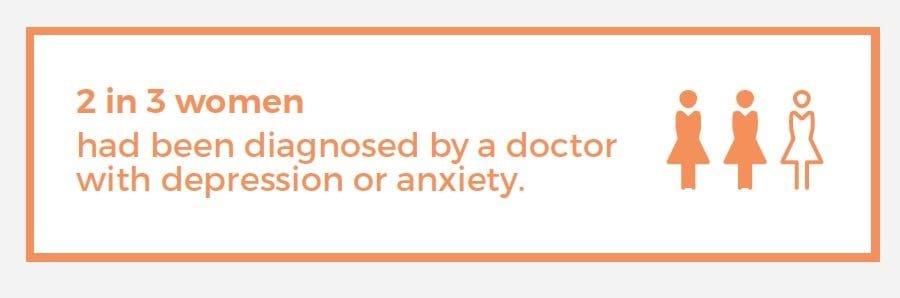
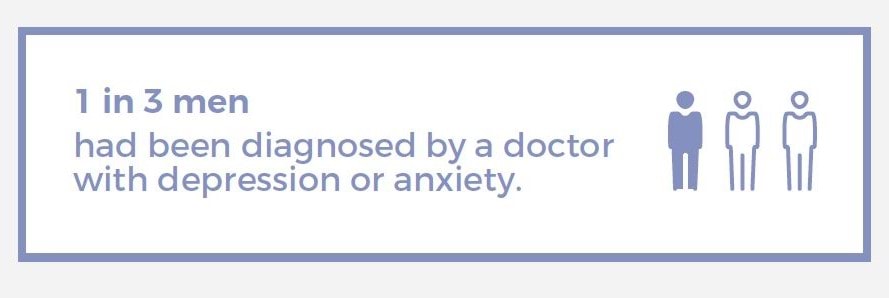
Source: 2017 Victorian Population Health Survey
The Royal Commission into Victoria’s Mental Health System (RCVMHS), which handed down its final report in March 2021, acknowledged family violence as a driver of mental ill health and provided a blueprint for a redesigned mental health system. We have seen little evidence of coordination between the mental health and family violence reforms, but we anticipate the implementation of several of the RCVMHS’s recommendations will improve the quality of and access to mental health services for family violence victim survivors. For example, the RCVMHS recommended a new approach to addressing trauma in Victoria, supported by a new statewide trauma service. This new approach will also include the placement of specialist trauma practitioners in each of 22 new Adult and Older Adult Area Mental Health and Wellbeing Services, along with the 13 new Infant, Child and Youth Area Mental Health and Wellbeing Services. We suggest ongoing coordination of the implementation of both sets of reforms will be essential, and many family violence sector stakeholders have called for the clear articulation of the mental health system’s role in victim survivor recovery.
“Children from families experiencing family violence should be overseen by a consistent and appropriately trained child psychologist, for the duration of their childhood."
Lily, victim survivor
As we raised in our Early Identification of Family Violence Within Universal Services report, patients often have close, trusting and extended relationships with their general practitioner, so it makes sense to use this connection for ongoing monitoring of a victim survivor’s wellbeing. However, as the Royal Australian College of General Practitioners has raised with us, the available Medicare items do not cover family violence, long consultations are not financially supported, and while victim survivors often present with both physical and mental health issues, Medicare does not allow GPs to bill for both mental and physical health on the same day.
The Royal Commission raised the need for Medicare reform, recommending:
The Victorian Government, through the Council of Australian Governments, encourage the Commonwealth Government to consider a Medicare item number for family violence counselling and therapeutic services distinct from a general practitioner mental health treatment plan. In the longer term consideration should be given to establishing a Medicare item number or a similar mechanism that will allow medical practitioners to record a family violence–related consultation or procedure and so more accurately ascertain the public cost of family violence. (Recommendation 105)
We suggested similar action in our Early Identification of Family Violence Within Universal Services report. We note that the creation of any new family violence–related Medicare item(s) would need to be accompanied by safety measures to ensure perpetrators on the same Medicare card would not be able to look up the card’s claims history and see that a family violence consultation had occurred.
Unfortunately, the National Plan to End Family Violence Against Women and Children does not mention the need for changes to Medicare to better allow GPs and others to support victim survivors, although it does acknowledge Medicare as an Australian Government system with a role to play in ending family violence. We suggest there is still an opportunity to highlight action in this area through the two action plans that will be developed to implement the national plan [relates to action 4].
“We need long-term access to mental health supports for victim survivors and their children and the opportunity for stability through stable housing, access to a stable income. Until we have stable basic needs – like safety, food and shelter – how can we recover?"
Jasmine, victim survivor
Peer support
Building on the discussion in other sections of this report about the potential role of a more structured lived experience workforce in the family violence sector, many victim survivors we consulted with told us of the healing power of connecting with their peers through lived experience groups like the Victim Survivors’ Advisory Council. It was an important part of their journey towards recovery. Sector stakeholders similarly spoke of the power of bringing victim survivors together for the purpose of building their peer connections and supporting their recovery, and they shared examples of effective peer support programs (see Box 6 for an example). However, these programs were locally driven and not centrally funded, which means victim survivor access to such programs is variable. The programs are also not always well-known and understood by other parts of the service system, even locally, which made it difficult to get referrals.
“Peer support is such a great support service. It facilitates both a connection back into the community but also the ability to reflect and express experiences in a safe place." - Heshani, victim survivor
“It helps to have people who can relate to you and know what you’ve been through." - Jasmine, victim survivor
There are also examples of child- and youth-focused group programs that contain a peer support element (see Box 7 for one example). As a Berry Street Y-Change Lived Experience Consultant powerfully stated:
Family violence is rarely seen or understood through the eyes of children and young people. Way too often, we are the ones you leave behind.
It would be worth considering whether and how such programs could be made available to support more children and young people who have experienced family violence to ensure they feel seen and heard [relates to action 6]. More broadly, we suggest there is likely great value in establishing peer support as a more consistent part of a suite of supports available to victim survivors as part of their recovery. One suggestion worthy of consideration was to have peer support groups running alongside all specialist family violence services.
“Often people have lived with a great deal of violence and control and doing basic things like washing, cleaning, cooking, and paying bills or general routine for everyday life is a struggle. I think starting from the beginning and working through general life would be helpful, it could even be a support group type environment, maybe even run by peer groups..."
Kelly, victim survivor
Box 6: The DAWN mentoring program
The Doncare Angels for Women Network (DAWN) mentoring program is a long-term support program for women who are recovering from the impacts of family violence. Trained volunteer mentors are matched to the women based on mutual interests, location and availability. The program aims to improve safety and build confidence and community connectedness among victim survivors. Mentors provide weekly support by assisting with access to services like financial counselling, women’s support groups, and court and legal services. They act as a source of companionship at a time when many victim survivors can feel isolated. This support spans 12–24 months. It has been estimated that over half of the volunteer mentors have had experience themselves of family violence, either directly or through friends or family members, and can help women navigate the system and learn what services are available to them.
Clients are referred to the DAWN program by family support workers, counsellors, emergency relief workers, women’s refuges, other welfare services and police. The program began in 2007, with Australian Government and philanthropic funding for the first two years. It has largely been funded by Manningham City Council since 2009; however, more recently, funding from the Ian Potter Foundation has allowed it to expand beyond the Manningham catchment to include the cities of Whitehorse, Maroondah, Monash, Boroondara, Knox and Banyule.
A 2016 evaluation of the DAWN program assessed the program’s impacts since its development in 2007. This found significant reductions in levels of depression, anxiety and stress for surveyed clients post the DAWN program. The women also generally reported feeling calmer, happier, more hopeful and that they were managing better. It also noted the positive side effect of improvements in the quality of life for the children involved, once the mothers felt supported and more confident.
Source: Based on advice provided by the Eastern Metropolitan Regional Family Violence Partnership and Doncare (2016), Doncare Angels for Women Network Evaluation Report 2007–2016.
Box 7: Feeling Visible pilot program for young people
WRISC Family Violence Support offers wraparound services and programs for children and youth living in the Central Highlands region. It is piloting a six-week, school-based, small group program – Feeling Visible – run by a registered art therapist. The program caters for students demonstrating the impacts of family violence. Students are engaged using an art-based, trauma-informed approach.
The program uses a peer support model to foster connections with others in the group who have had similar experiences. It enables them to build confidence and connections with others in a shared space to develop a personal language to describe their experiences.
The evaluation of the pilot at one school showed that the vast majority of participants felt a strong sense of safety while participating in the group sessions, with one student commenting that their ‘favourite part was going around the circle and talking about it together’.
The facilitator of one of the pilot programs reported that participants, through peer support, are developing and learning ways to understand their experiences and what they need in order to heal, enabling them to make healthy choices when feeling overwhelmed and notice what their bodies are telling them about their physical and emotional safety.
One of the benefits identified through the evaluation came from one of the pilot school’s mental health practitioners:
I have observed the students being more connected to each other and to wellbeing, breaking down some of the stigma around family violence and help seeking in general, they have felt seen and validated in their experiences [and] they have had a positive experience of a therapeutic relationship, having a chance to have ‘voice and choice’, and they have learned gently and in a non-threatening way about family violence.
Source: Based on information provided by WRISC Family Violence Support, including a program evaluation.
Updated