
After being assessed by Safe Steps and/or The Orange Door, victim survivors can be referred to specialist family violence services for case management support (adult male victim survivors engaging with the Victims of Crime Helpline can be referred to the Victims Assistance Program). Family Safety Victoria has also advised that victim survivors can self-refer to specialist family violence services as part of a ‘no wrong door’ principle. Stakeholders overwhelmingly told us, however, that high levels of demand pressure on the system mean that very few victim survivors will receive case management. We have not been able to obtain any data that describes how many victim survivors are referred to case management, how many receive it, nor how long they wait to commence case management support.
Case management practice
The case management that specialist family violence services provide is now guided by case management program requirements, approved and released in December 2021. The sector was already guided by a code of practice developed by Safe and Equal, which includes practice principles such as person-centred empowerment, inclusion and equity, and child-centred practice. However, the new program requirements represent the first time a case management ‘manual’ has been provided and describe what specialist family violence services need to do to provide high-quality case management services for victim survivors.
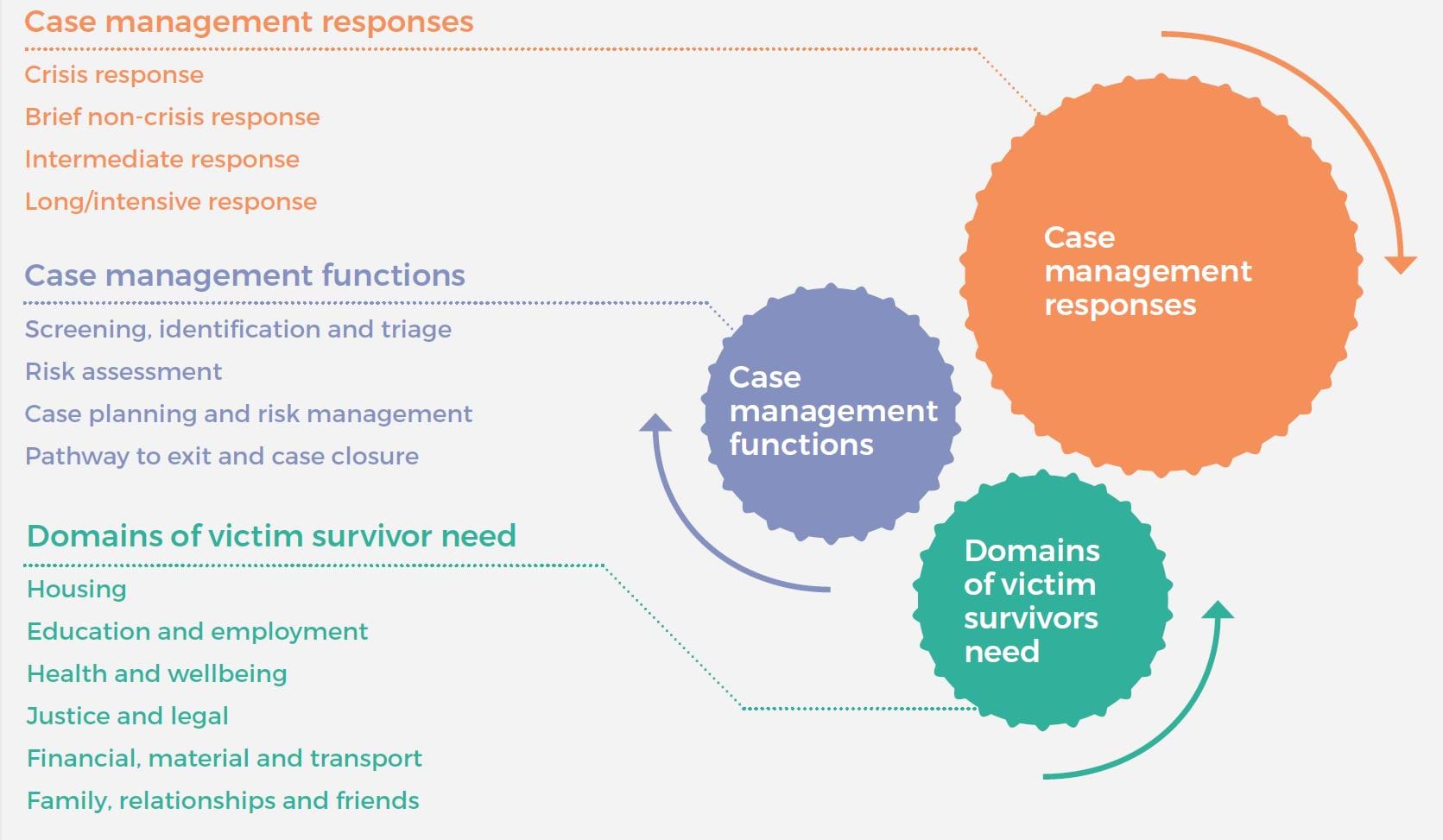
The program requirements clearly outline the types of responses specialist services deliver (from crisis response to a long-term intensive response), the particular functions these services carry out (including risk assessment and case planning) and a series of domains in which victim survivors might need support (including housing and legal). These aspects of case management are outlined in Figure 8.
While there are no timeframes attached to the response types outlined in the program requirements, stakeholders were consistent in telling us that the longest duration of support would normally be three months, with most people receiving around six to eight weeks of case management support. There was concern that three months of case management support for those in the greatest need is insufficient, and anecdotally, case managers feel they are ending their support before victim survivors are ready and able to sustain their own recovery.
It is positive to see the domains of support outlined so clearly in this document, as these reflect the areas of support the Royal Commission explained were essential for victim survivor recovery. Stakeholders, including victim survivors, confirmed this. The challenge, as always, will be to ensure frontline practice reflects the high-level requirements in the context of ongoing demand pressure and workforce challenges. The documentation we reviewed from Family Safety Victoria suggests a gradual process of alignment with the requirements, with support available from Family Safety Victoria and Safe and Equal, and some alignment funding provided to services. Full alignment is expected by the end of 2023. We understand that independent review bodies will examine organisations’ systems, policies and services for their alignment with these requirements as part of broader reviews of compliance with the Human Services Standards. However, we suggest that ongoing monitoring of practice and outcomes, accompanied by appropriate support, will be essential to effectively implement these program requirements.
This ongoing monitoring should consider how different groups in the community are experiencing the service system. For example, there was a perception that victim survivors who wish to remain with the perpetrator will not be supported by specialist family violence services, but the case management program requirements clearly stipulate that such clients are eligible for a brief non-crisis response or an intermediate response.
Figure 8: Program requirements for specialist family violence services
Family violence case management – supply and demand
Although we have been unable to obtain data on the number of referrals from The Orange Door to specialist family violence services and the wait time to access these services, stakeholders consistently told us about major challenges in connecting victim survivors with services [relates to action 14]. We suggest that without this critical data on referrals and wait times for access, it is impossible for Family Safety Victoria to accurately monitor and model demand for services and plan and allocate resources.
Through recommendation 39, the Royal Commission recommended that:
The Victorian Government, on the basis of demand forecasting, provide sufficient funds to specialist family violence services and Integrated Family Services to allow them to support people referred by a Support and Safety Hub, maintain their safety and help them until their situation has stabilised and they have the support necessary to rebuild and recover from family violence.
Safe and Equal advised us that while specialist family violence services have received large funding increases over recent years, demand is too high for services to be able to meet it [relates to action 13]. It pointed out that enormous investment has gone into creating The Orange Door as the main intake point for the system, but there hasn’t been a sufficient increase in building the service system beyond The Orange Door to ensure a smooth flow of referrals. This means that there are long wait times, leading to people dropping out of the system, or victim survivors’ circumstances changing substantially by the time they connect with a service. This can mean victim survivors have to repeat their story so a new risk assessment can be completed. It can also mean that victim survivors have disengaged from services or are not safe to engage with support by the time a specialist service makes contact with them.
Feedback from the Statewide Family Violence Integration Advisory Committee is that one of the aims of the reform program was to intervene earlier and avoid victim survivors reaching the crisis stage. Consistent with this, the new case management program requirements are clear about the importance of responding to early help-seeking behaviour:
A victim survivor's early help seeking provides a crucial opportunity for preventing an escalation of risk to a serious level of crisis through effective screening, identification and triage, mechanisms for rapid secondary consultations, responsive referral pathways between services and inter-agency partnership …. It is crucial that specialist family violence services recognise and act upon this opportunity when responding to referrals, and especially self-referrals.
Family Safety Victoria has advised that once victim survivors have been assessed at The Orange Door, there are no specific criteria for referral to case management; instead, referrals are said to be based on a discussion with the victim survivor about whether case management is required. Numerous stakeholders told us, however, that in practice only the highest risk clients, and sometimes only those who are considered to be in crisis, are getting through to case management. We heard that case management services previously worked with a greater mix of clients but that their clients are now limited to those at the crisis end, with higher risk and complexity. We understand that in a system under pressure, there is a need to prioritise clients according to need, but we suggest more needs to be done to ensure all victim survivors are getting support to meet their needs and avoid escalation and future incidents, thereby reducing future pressure on the system.
Because of the long wait time for case management support from specialist family violence services, The Orange Door is left ‘holding’ clients, which diverts resources and creates further delays for new referrals.
Stakeholders also shared examples of victim survivors (and risk) being held by a range of other services, many of which are often facing similar demand challenges. For example:
- A maternal and child health family violence worker said she often works outside her scope of work to hold clients facing long (sometimes many months) waits to access specialist services. She does her best to support clients – for example, in applying for an intervention order – but does not feel well trained or supported in doing so. She suggests access to secondary consultations would help her feel more confident supporting clients in this way.
- The Department of Justice and Community Safety advised us that Consumer Affairs Victoria workers are now identifying and assessing risk but are finding that the lower risk referrals are not getting through for specialist support and are therefore left ‘holding the risk’. Many workers still lack confidence in this area, but this confidence is expected to improve as MARAM continues to be rolled out.
- An AOD service provider told us that AOD workers are picking up more of the family violence risk assessment and management that specialist services would otherwise be doing because of the backed-up family violence system. This is said to be placing an extra clinical and emotional burden on AOD staff, leading to burnout.
Sexual Assault Services Victoria advised that with the overall pressure on the family violence response system in Victoria, and imperative to prioritise those at greatest immediate risk, member organisations often struggle to refer victim survivors who are not at immediate risk for family violence counselling and case management. This means that opportunities to reduce risk through early intervention are missed. In addition, we understand that practitioners at The Orange Door are commonly referring to alternative services, even in high-risk cases, because of the demand pressure on specialist family violence services. Such alternative referral pathways include family services and general counselling services. One principal strategic advisor said those services are being flooded with referrals and that they cannot keep up, nor do they have the specialist expertise required. The Department of Justice and Community Safety’s Victims Assistance Program is also increasingly receiving referrals for female victim survivors of family violence from The Orange Door and specialist family violence services. While each Victims Assistance Program provider was recently funded for a position to lead family violence practice due to this increase, the program is designed to be a generalist response for victims of crime.
As suggested in our Early Identification of Family Violence Within Universal Services report, there is a need for a clear model for referral pathways and secondary consultations to support staff in universal health and education services that are encountering clients experiencing family violence [relates to action 1]. This could sensibly extend to other services that are frequently ‘holding’ victim survivors while they await support or directly supporting victim survivors who cannot access specialist services. The model could:
- describe the interface between The Orange Door, specialist family violence services, the Victims Assistance Program and other high-frequency referral points
- clearly outline referral pathways and how decisions about referrals should be made
- clearly outline secondary consultation options
- consider how the needs of particular groups can best be met, such as trans and gender diverse people, and migrant and refugee women, who may find it more difficult to have their needs met by family violence services, particularly in regional areas.
Importantly, consideration must be given to the capacity of services to respond to referrals and secondary consultations.
Stakeholders were clear that the ability for the specialist family violence system to meet demand means that many victim survivors do not receive the type and duration of support they need, and therefore end up cycling back through the system as their situation continues or worsens. We suggest further analysis should be undertaken to determine how boosting the specialist family violence response for more victim survivors would help to reduce overall demand by meeting people’s needs the first time, given the strong feedback we’ve received that many victim survivors are not receiving the support they need until they meet the system’s definition of crisis.
As suggested in the previous chapter, it would be highly beneficial to systematically track victim survivor journeys through the system including referrals, wait times for services, services provided and outcomes [refers to action 15]. We acknowledge that this is currently extremely difficult because each part of the system is tracking data differently and using incompatible information systems [refers to action 14]. In the meantime, we support more targeted, manual analysis of client journeys, including an emphasis on whether or not their needs have been met (as measured against agreed indicators). This will provide a clearer picture of where victim survivors are being referred and their service system experiences.
Victims Assistance Program for adult male victim survivors
As discussed previously, male victim survivors generally have a different service pathway from other victim survivors. After engaging with the Victims of Crime Helpline, they can be referred to the Victims Assistance Program, which is delivered by a selection of agencies in the community such as cohealth and Anglicare Victoria. It provides ‘case management services comprising practical support, criminal justice advocacy and therapeutic interventions to victims of crime throughout Victoria’. However, based on data provided by the Department of Justice and Community Safety, only a very small proportion of males referred to the Victims of Crime Helpline by police end up being referred to the Victims Assistance Program (6.5 per cent in 2019–20; see Table 3).
Table 3: Outcomes of Victims of Crime Helpline contact with males referred by police as Affected Family Members on Family Violence Reports, 2019–20
| Contact action wrap-up | Intimate partner violence | Non-intimate partner violence | Total | Percent (%) |
|---|---|---|---|---|
| Client not reached | 1708 | 1400 | 3126 | 18.0% |
| Client took information for consideration | 1002 | 1044 | 2055 | 11.8% |
| Client declined support | 817 | 1173 | 1996 | 11.5% |
| Client referred to Victim Assistance Program | 503 | 621 | 1129 | 6.5% |
| Client already linked with supports | 323 | 296 | 622 | 3.6% |
| Client referred to other service | 164 | 63 | 227 | 1.3% |
| Other | 3661 | 2168 | 5848 | 33.7% |
| N/A or Missing | 1308 | 844 | 2366 | 13.6% |
| Total | 9486 | 7609 | 17369 | 100.0% |
Source: Department of Justice and Community Safety (2020): Victims of Crime Helpline: Annual Data Report 2019-20.
However, the Victims Assistance Program is generalist in nature. The Centre for Innovative Justice has completed a thorough review of victim services in Victoria, including the Victims Assistance Program, and found that:
Despite a number of skilled and highly dedicated practitioners supporting delivery of the program, and some promising innovations at the local level to meet clients’ needs more effectively, demand pressure on the [Victims Assistance Programs] and a lack of rigorous, outcomes-focussed performance management has resulted in significant variability in terms of the nature and quality of service provision.
To manage high levels of demand, the victims services review found that organisations delivering the Victim Assistance Program were narrowing their service scope and often focusing primarily on practical and criminal justice tasks. They have access to brokerage funding for their clients, and this is primarily used for counselling but can also be used to fund practical and safety supports. These organisations can also contact relevant regional agencies to access Flexible Support Packages for male victim survivors; however, the Department of Justice and Community Safety has advised that, in practice, males are less likely to receive support this way because they will generally be deemed to be at lower risk than female victim survivors.
Some stakeholders told us that the lack of referral options means male victim survivors are sometimes referred to men’s services such as the Men’s Referral Service, Boorndawan Willam Aboriginal Healing Service and Mullum Mullum Indigenous Gathering Place [refers to action 8]. However, these services are designed for men using violence, and the organisations are not funded to work with victim survivors. Boorndawan Willam Aboriginal Healing Service does hold male victims in case management but is concerned that this risks labelling them a perpetrator.
The victim services review called for a more specialised service for male victim survivors, delivering more holistic, needs-based responses. It stated:
As the primary service response for male victims of family violence, [Victims Assistance Programs] need to incorporate a specialised response that more closely reflects supports available to women and children. This includes expanded eligibility criteria to align with legislative definitions of family violence; a greater brokerage allocation to reflect the lack of services, including crisis accommodation, for this cohort; and an appropriate level of specialisation to respond to male victims of family violence, including male children; older men who are victims of elder abuse; and gay, bisexual and transgender men.
Updated